Download to read offline

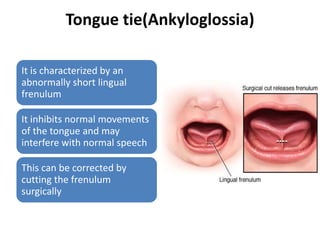
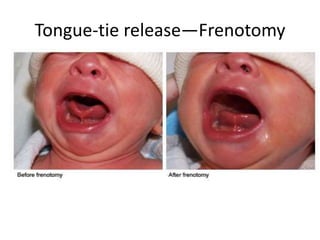
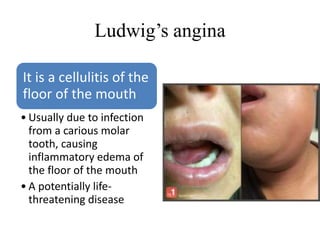
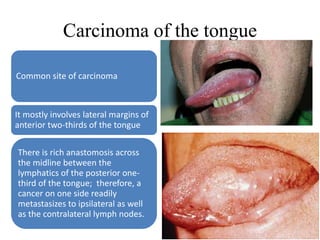



1. Tongue-tie is characterized by an abnormally short lingual frenulum that can inhibit tongue movement and speech, and is corrected by surgically cutting the frenulum. 2. Ludwig's angina is a potentially life-threatening cellulitis of the floor of the mouth usually caused by a dental infection that causes swelling. 3. Carcinoma of the tongue most commonly involves the lateral margins of the front two-thirds of the tongue and can readily metastasize to lymph nodes on both sides.




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




