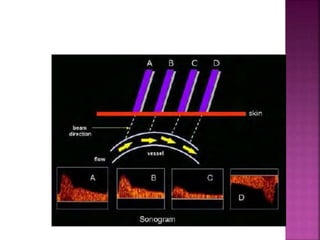
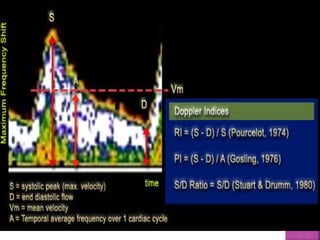
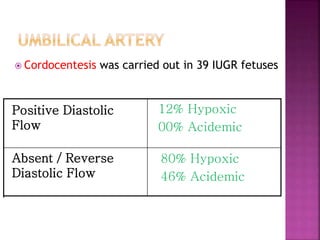
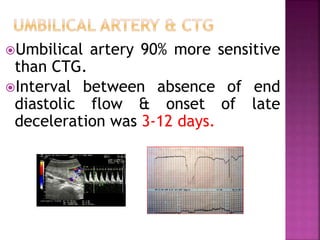
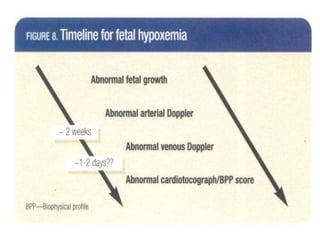
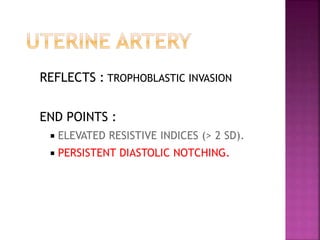
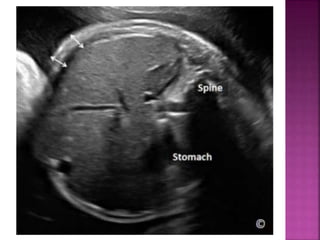
This document discusses intrauterine growth restriction, fetal doppler, and macrosomia. It defines these conditions and outlines their causes, diagnostic techniques like doppler ultrasonography, and implications. Doppler uses ultrasound to measure blood flow and has been used since 1977 to study umbilical artery flow velocity. It is useful for assessing fetal well-being and risk of complications like neonatal intensive care unit admissions or brain injuries. The document also details ultrasound findings and considerations for at-risk growth-restricted or large fetuses.
































![H:\Physiological Changes In Pregnancy[2]](https://cdn.slidesharecdn.com/ss_thumbnails/hphysiologicalchangesinpregnancy2-100305140624-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)























![Umbilical artery doppler [1]](https://cdn.slidesharecdn.com/ss_thumbnails/umbilicalarterydoppler1-210517112207-thumbnail.jpg?width=640&height=640&fit=bounds)













































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






