Downloaded 127 times
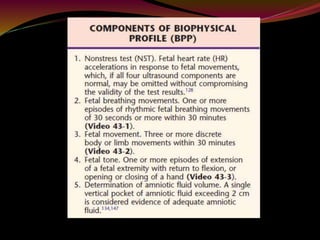
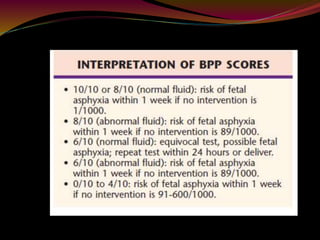
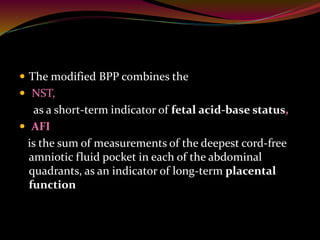
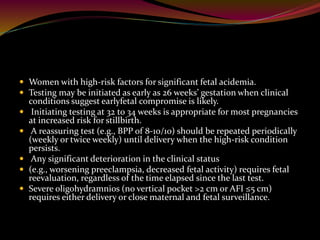
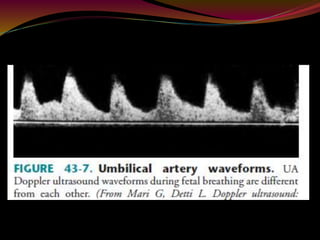
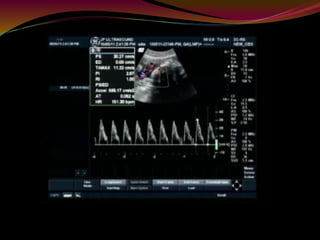
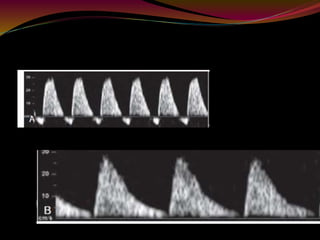
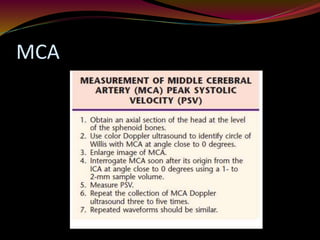
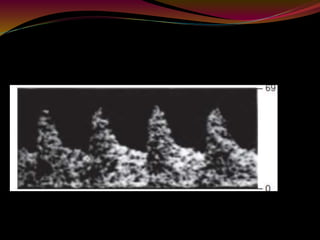
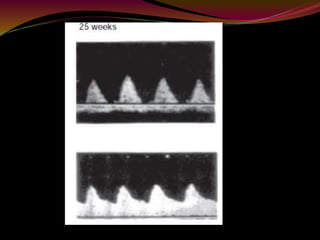
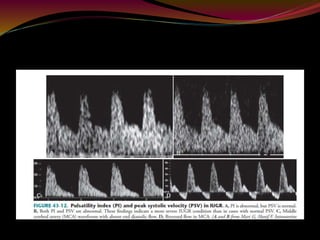

This document discusses various methods for assessing fetal well-being, including the biophysical profile (BPP), modified BPP, Doppler ultrasound of the umbilical artery (UA) and middle cerebral artery (MCA), and fetal breathing movements. The BPP assigns scores based on 5 components to evaluate fetal condition. Doppler ultrasound of the UA and MCA can identify fetuses at risk, with abnormal UA Doppler indicating uteroplacental insufficiency and intrauterine growth restriction. MCA Doppler detects the brain-sparing effect in which blood is redistributed from the UA to the brain in compromised fetuses.






























![Umbilical artery doppler [1]](https://cdn.slidesharecdn.com/ss_thumbnails/umbilicalarterydoppler1-210517112207-thumbnail.jpg?width=640&height=640&fit=bounds)













































