Downloaded 1,243 times
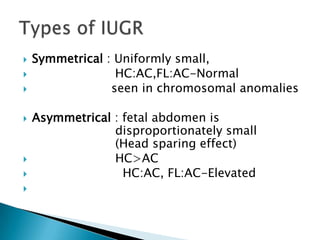
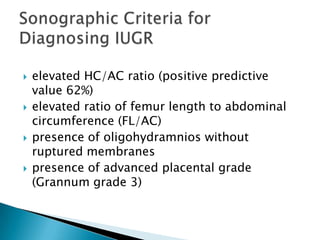
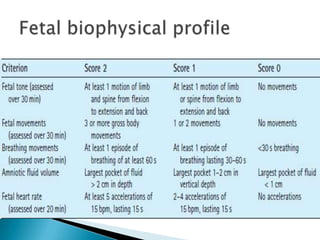
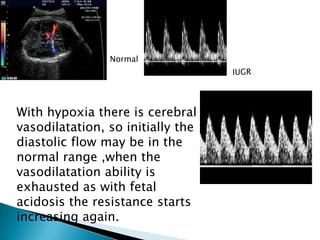

The document discusses Doppler ultrasound findings for a 25-year-old pregnant female with uncontrolled hypertension. Key findings include oligohydramnios, elevated head circumference to abdominal circumference ratio, and abnormal Doppler readings of the umbilical artery, middle cerebral artery, and ductus venosus indicating fetal hypoxia and intrauterine growth restriction. The summary provides an overview of the patient details and significant ultrasound findings reported in the document.












































![Umbilical artery doppler [1]](https://cdn.slidesharecdn.com/ss_thumbnails/umbilicalarterydoppler1-210517112207-thumbnail.jpg?width=640&height=640&fit=bounds)





















![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
