Downloaded 84 times
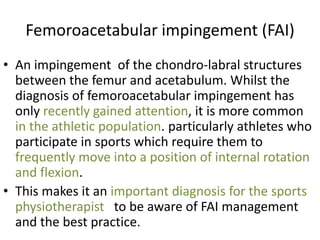
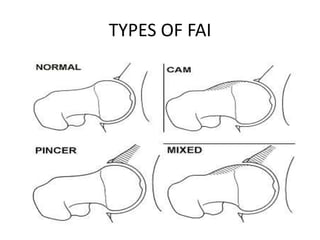
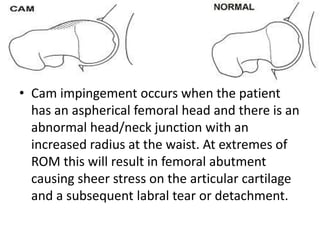
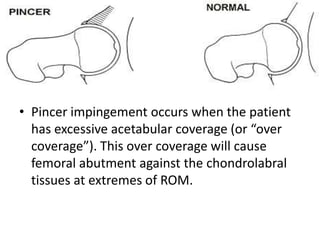
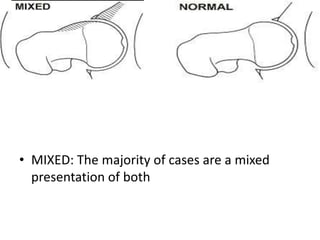

This document discusses femoroacetabular impingement (FAI), a condition where the femoral head and acetabulum abnormally contact each other, from the perspective of a sports physiotherapist. It describes the two main types of FAI - cam impingement caused by a nonspherical femoral head, and pincer impingement caused by excessive acetabular coverage. Most cases involve a mix of both. Conservative physiotherapy management focuses on reducing inflammation, strengthening muscles, and gentle stretching. Surgical intervention like arthroscopy may be considered if conservative treatment fails to allow athletes to return to play.















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

