Download as ODP, PPTX




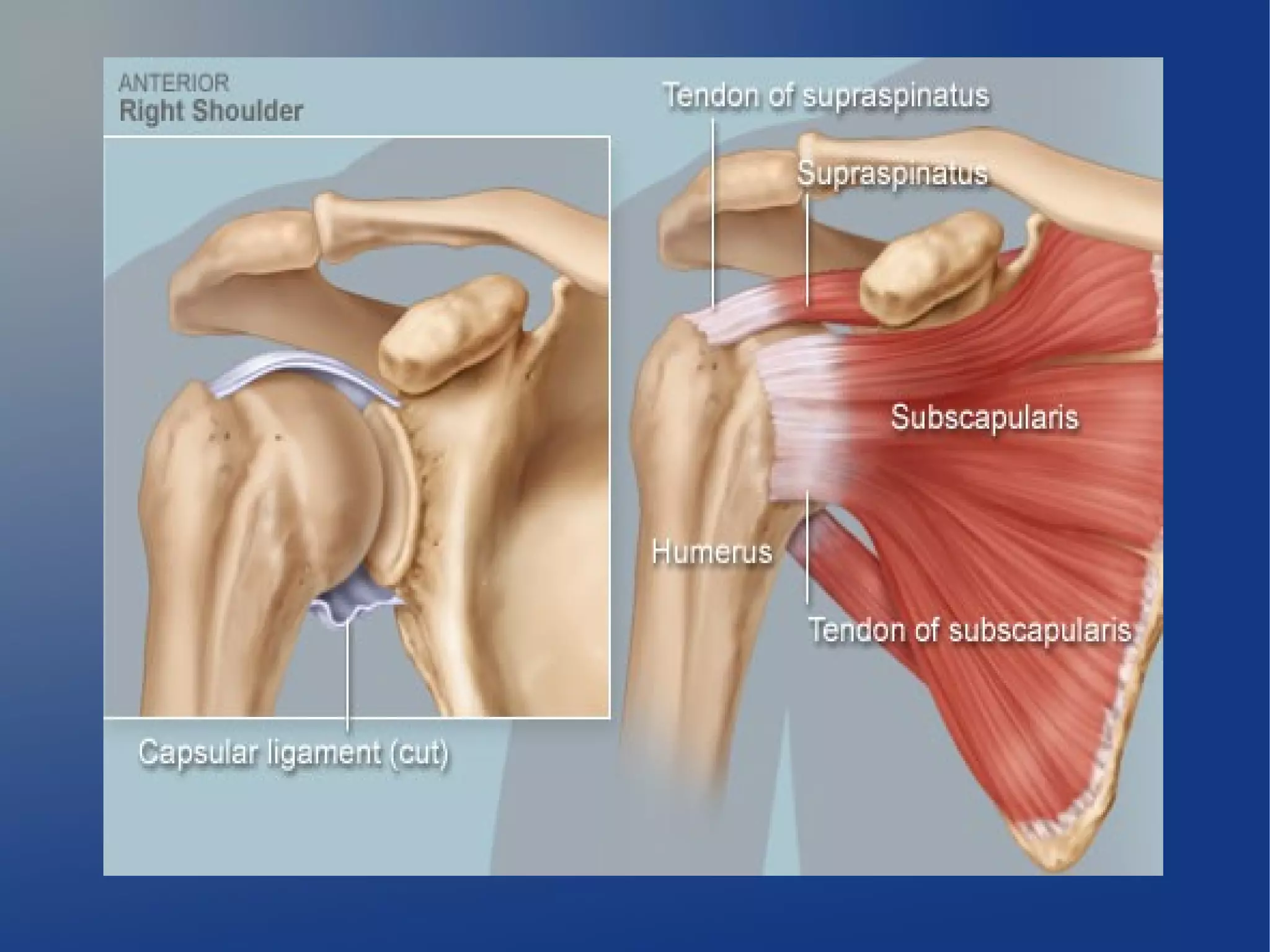


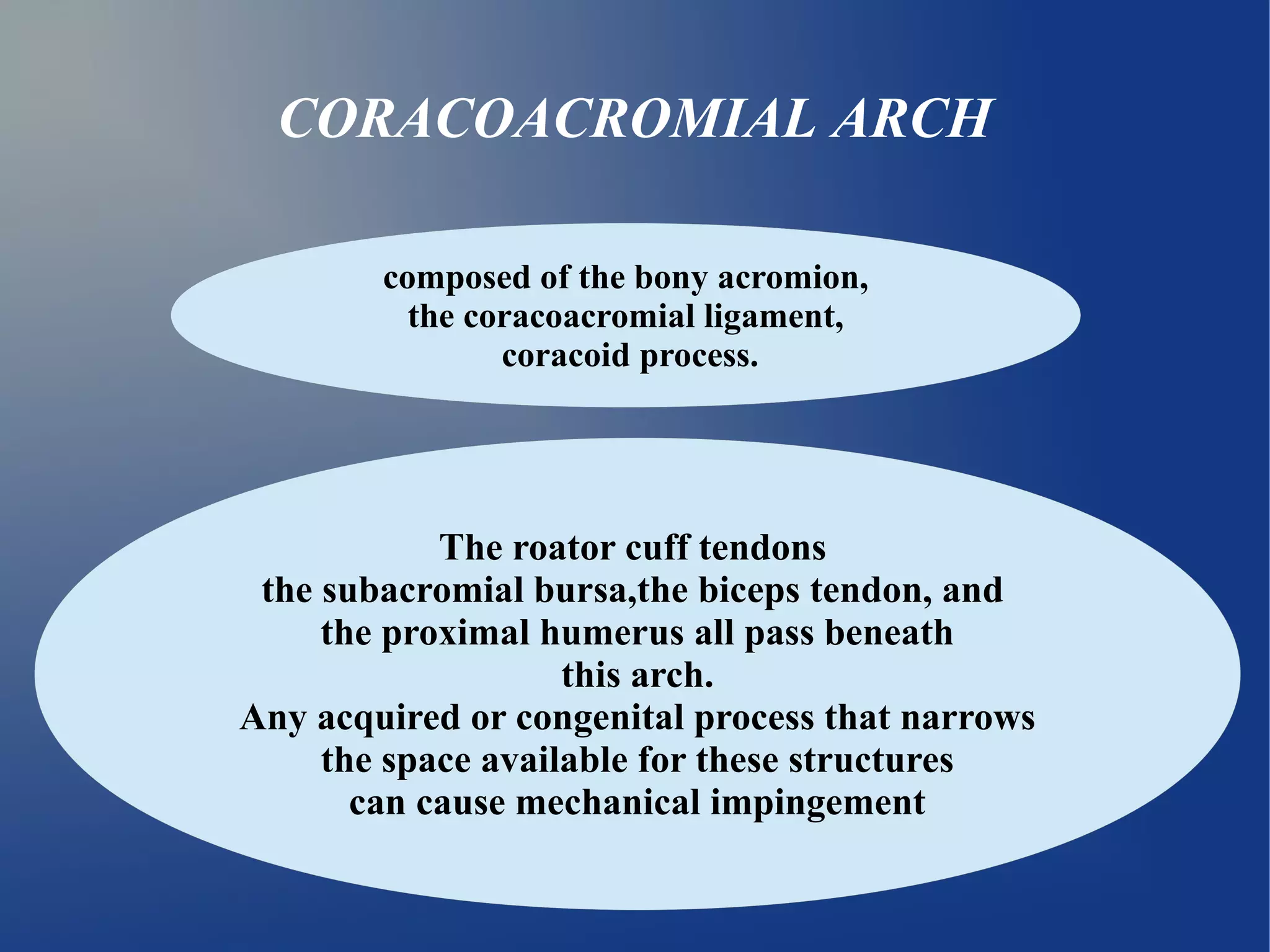

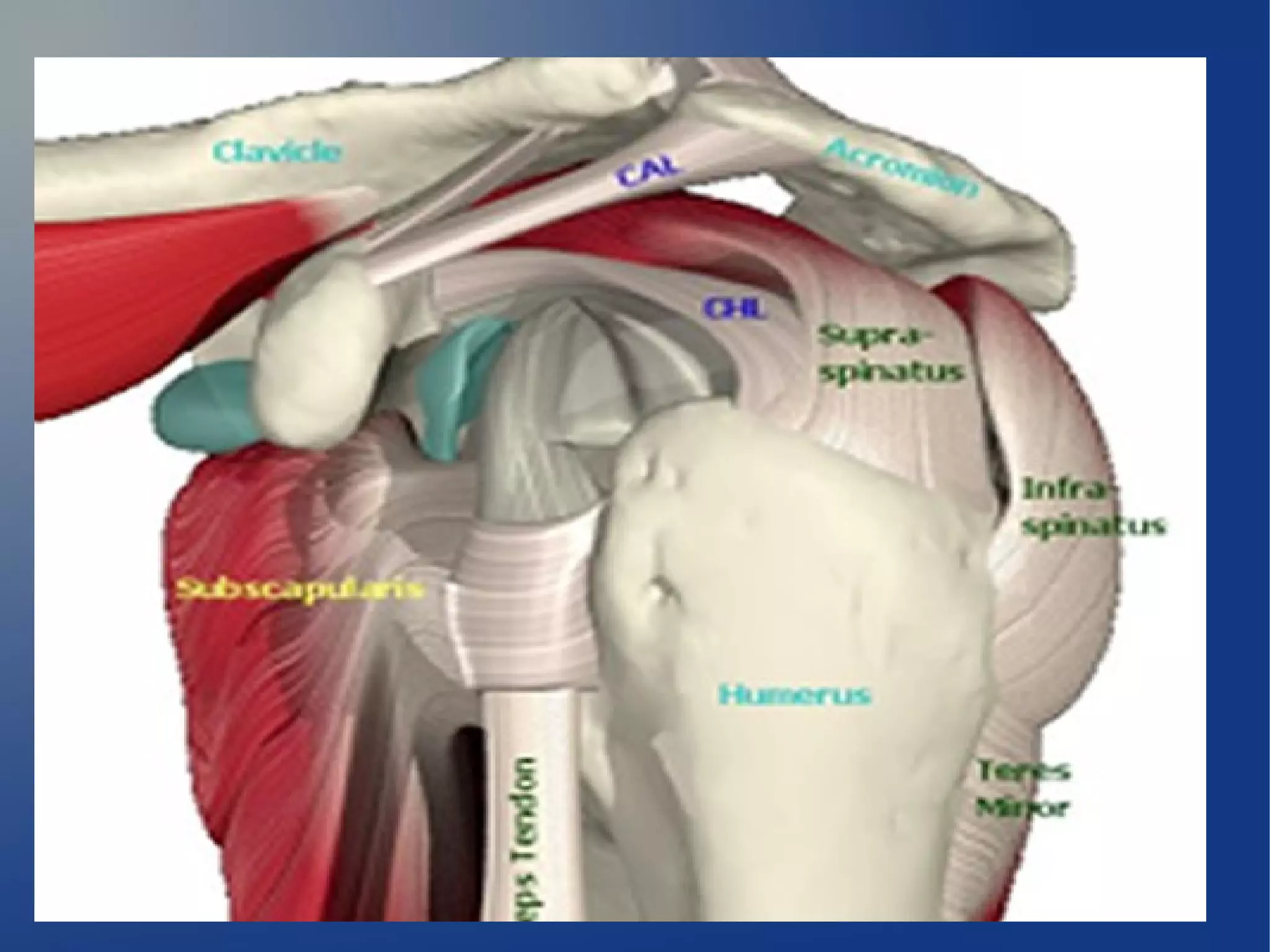




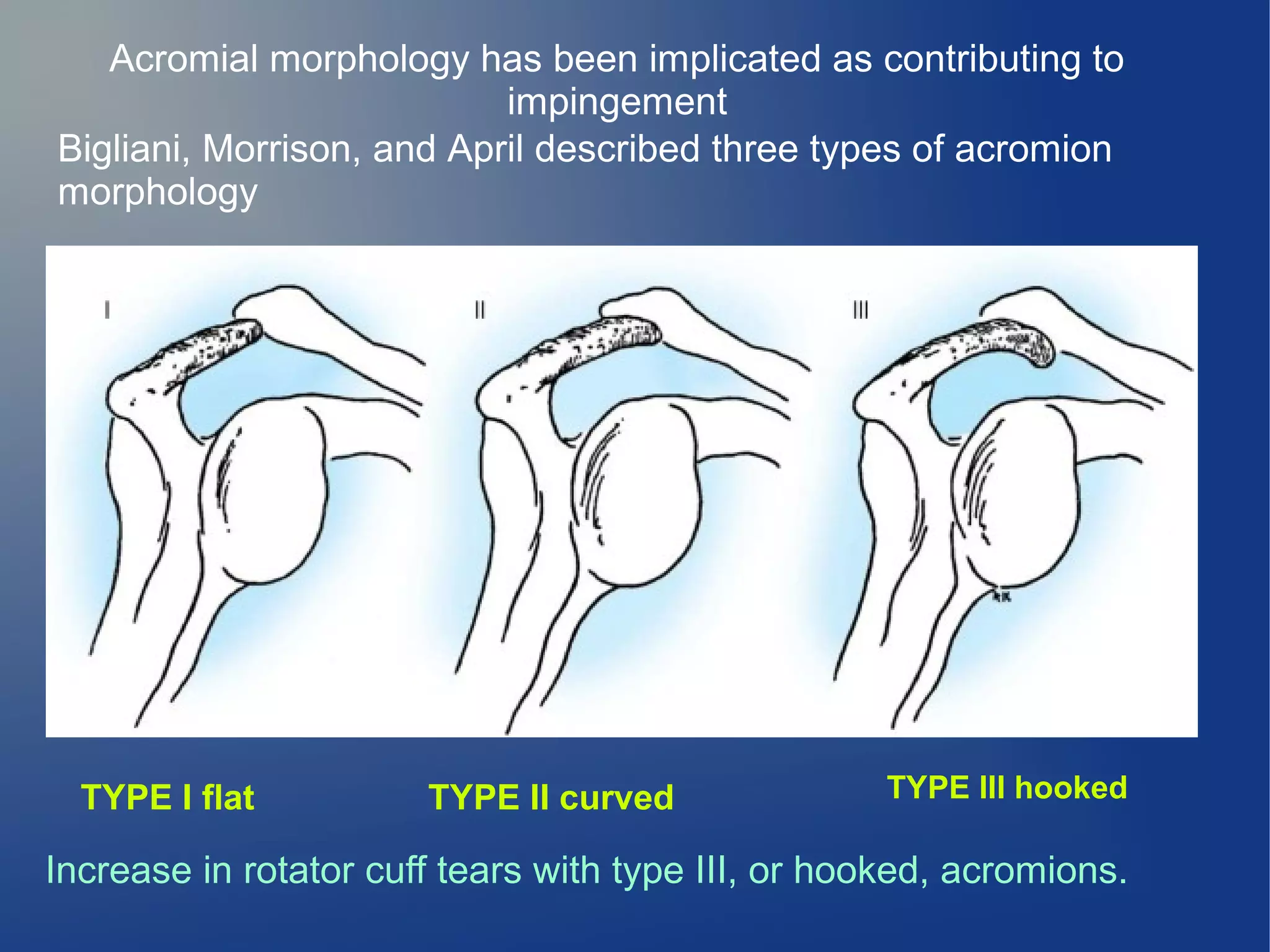
















































1) Shoulder impingement syndrome is caused by compression of the rotator cuff tendons between the acromion and humeral head. It commonly results from a hooked acromion or inflammation/thickening of the tendons. 2) Treatment begins conservatively with anti-inflammatories, cortisone injections, and physical therapy. If unsuccessful, surgery such as open or arthroscopic acromioplasty is recommended to remove bone spurs and widen the space. 3) Acromioplasty involves detaching the deltoid muscle, removing the coracoacromial ligament and anterior portion of the acromion, and inspecting/repairing any rotator






![ROTATOR CUFF[4273].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rotatorcuff4273-221222051719-751991ae-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































