Downloaded 91 times

![• Many medications given to neonates have the
potential to injure when an extravasation
occurs.
• An extravasation is described by the Infusion
Nurses Society (INS) as the inadvertent
administration of a vesicant solution or
medication into the surrounding tissues.[1]](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-2-2048.jpg)

![Infiltration Is Common Among Neonates
• The peripheral intravenous (PIV) catheter is the
most used vascular access device for the
administration of medications in hospitalized
neonates; however 95% of PIV catheters are
removed due to complications such as leaking,
occlusion and infiltration.[4]
• Infiltration rates among neonates are as high as
57%–70% with extravasation occurring in 11–
23%.[5] Both infiltration and extravasation are
destructive](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-6-2048.jpg)




![The preterm and sick neonate is more
susceptible to skin injury and complications
from extravasation injury than their mature,
healthy counterparts.
• Their immature skin structures,
• flexible subcutaneous tissue,
• small blood vessels and poor venous integrity
increase the risk of complication from
venipuncture and IV infusions.[5,8]](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-11-2048.jpg)
![Inflammation in the Premature Infant
• The neonatal immune system is poorly
regulated compared to adults and
dysregulation is magnified when neonates are
born early.[11-13] While intravenous therapy is
necessary in this population, it is not without
its risks.](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-13-2048.jpg)
![• which is common in prematurity, or the
inflammatory assault is severe, endothelial
dysfunction leads to programmed cell death
(apoptosis).[16]
• The load of oxidative stress in premature infants
is especially of concern as it has been linked to
various neonatal morbidities including
necrotizing enterocolitis,[16,17] retinopathy of
prematurity,[18-20] and chronic lung disease.[16,21-
23]](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-15-2048.jpg)

![The Neonatal Intensive Care Unit
(NICU) Nurse's Role
• NICU nurses monitor the PIV site with
vigilance to aid in early identification of
infiltration and extravasation and prevent this
type of injury whenever possible. Identifying
an infiltration may be difficult, even for the
most experienced nurse.[10]](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-17-2048.jpg)

![Potential Origins of Infiltration
• There is a supposition that an infiltration or
extravasation is caused by IV catheter dislodgement or
puncture of the vein during insertion or during
handling of the infant.
• Chemical composition of medications also impacts risk
of vein rupture.[5]
• The vein's tolerance to an infusion is affected by the
osmolality and pH of the vesicant, the duration of the
exposure, and irritation to the endothelial cells.[4]
• An additional factor in causing a cannulated vessel to
rupture and leak is the pressure in which the
medication is being delivered by the infusion pump.[3,5]](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-19-2048.jpg)
![Irritants and Vesicants Given to
Neonates
• ntravenous medications can be divided into
three major subcategories: 1) non-vesicants,
2) irritants, and 3) vesicants. In order for an
infiltration to be a true extravasation, the
offending agent, by definition, must be a
vesicant. There are a number of different
qualities that affect the potential for a
medication to result in tissue damage. These
include, but are not limited to: osmolarity, pH,
direct medication effects and solubility.[27]](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-20-2048.jpg)
![• ntravenous medications can be divided into
three major subcategories: 1) non-vesicants,
2) irritants, and 3) vesicants. In order for an
infiltration to be a true extravasation, the
offending agent, by definition, must be a
vesicant. There are a number of different
qualities that affect the potential for a
medication to result in tissue damage. These
include, but are not limited to: osmolarity, pH,
direct medication effects and solubility.[27]](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-21-2048.jpg)

![Nursing Actions to Prevent Vascular
Injury
• The best method to decrease complications of PIV
therapy is to prevent them in the first place.[2]
• Serious complications are not entirely preventable, but
following recommended standards of IV therapy is the
best approach for avoiding complications.[3]
• The decision to place a peripherally inserted central
catheters (PICC) or central venous lines (CVL) might be
needed if vascular access is difficult or long-term
parenteral therapy is planned. However](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-23-2048.jpg)



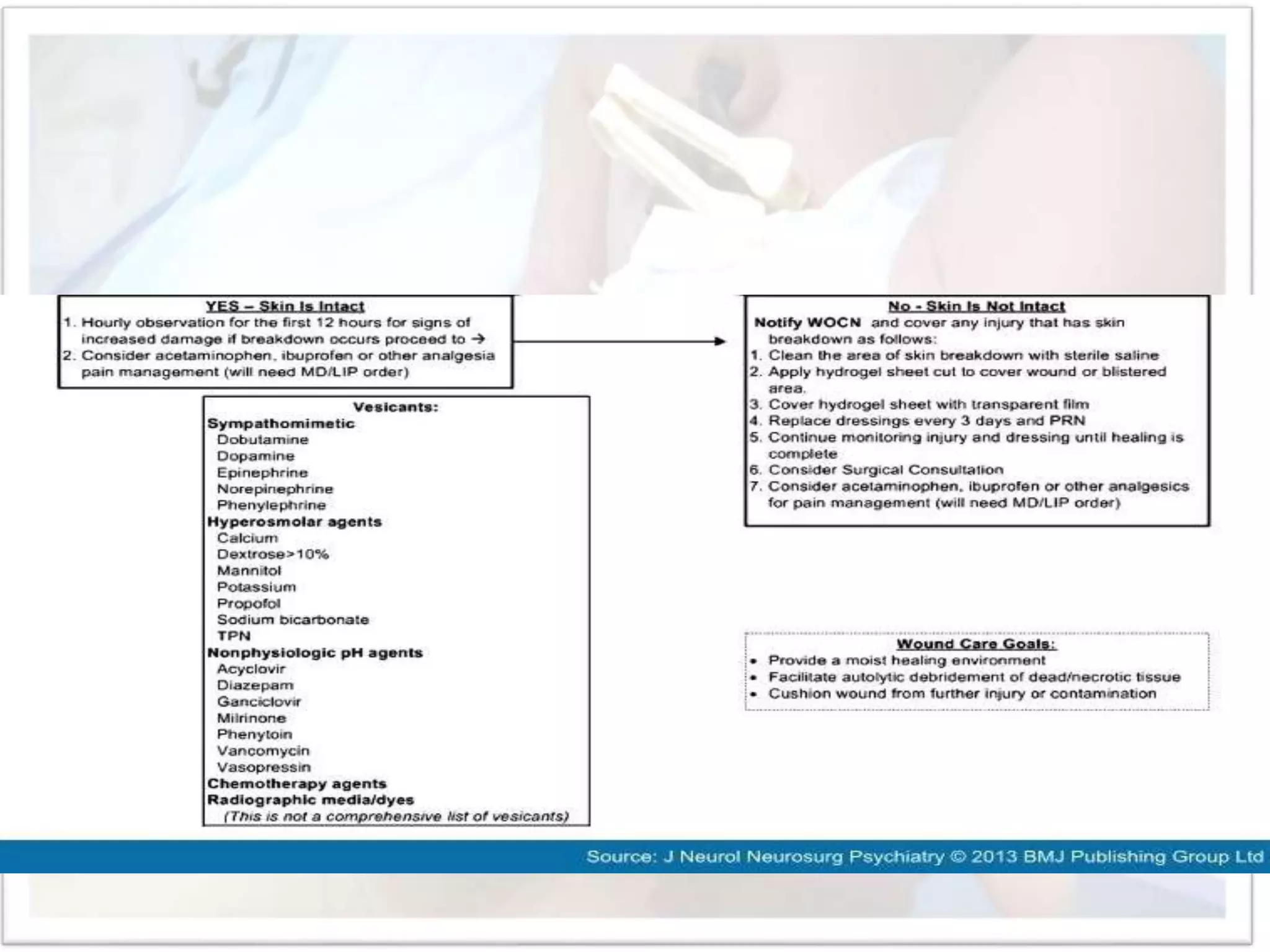
![Key Actions to Minimize Injury When
Extravasation Occurs
• Once an infiltration or extravasation is
discovered, immediate treatment is the key to
preventing progressive damage from the
vesicant.[2]
• Treatment decisions are based on the size and
appearance of the injury, type of IV infusing,
duration of exposure and location.[8] Protocols
and algorithms can be used to assist nurses in the
steps needed to minimize the potential damage
and start the treatment process.](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-27-2048.jpg)
![• Stopping the infusion and elevation of the extremity is
the first actions followed by placement of a saline
soaked gauze or prepackaged normal saline pad.
• The saline draws out the vesicant, and impedes a scab
from forming to allow fluid to leak out.
• Gently squeezing the fluid from the open insertion site
can also help to remove the offensive agent.[8] While
the saline soaks are held in place, assistance with the
various tasks that are required for treatment may
require additional personnel.](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-28-2048.jpg)












![Phentolamine
• Phentolamine is an antidote that will counteract the effect of
vasoactive agents such as dopamine, epinephrine, norepinephrine
and phenylephrine.[8] These medications result in vasoconstriction
via stimulation of alpha-receptors.
• Phentolamine acts to block the activity of alpha-receptors and
subsequently will help relax vascular smooth muscle. This will
improve circulation in the area of the extravasation and thus
decrease ischemia and cell death. Phentolamine can also be utilized
for vasopressin or dopamine extravasation.[28]Phentolamine should
be administered within 12 hours of initial exposure but
administration should occur as soon as possible. Prepare a 0.5 to 1
mg/mL solution and administer 0.1 mg/kg (to a max of 2.5 mg in
neonates,](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-43-2048.jpg)
![• Nitroglycerin Ointment (2%)
• Nitroglycerin 2% is an option to treat extravasations.[8]Nitroglycerin
acts to relax smooth muscle resulting in arteriolar, arterial and
venous vasodilation that results in increased capillary blood flow,
counteracting the effects of vasoactive medications. This will help
to reverse tissue ischemia and cell death. In the neonatal
population, there is a case report describing the use of 1 inch of 2%
nitroglycerin ointment for treatment of a dopamine extravasation,
located in the dorsum of the left hand, in a 1.8 kg 34 week preemie.
This resulted in return of circulation within a few minutes. Of note,
treatment was started almost 12 hours after the extravasation was
initially noted and patient had no significant change in
hemodynamics.[33]](https://image.slidesharecdn.com/extravasationinneonate-170325120223/75/Extravasation-in-neonate-44-2048.jpg)






1) An extravasation occurs when a vesicant medication or solution is inadvertently administered into the surrounding tissues, potentially causing tissue injury. This is a common complication among neonates receiving intravenous therapies. 2) The NICU nurse plays an important role in monitoring intravenous sites for early signs of infiltration or extravasation and preventing injury. If extravasation occurs, immediate treatment is needed to minimize damage, such as stopping the infusion and applying saline compresses. 3) Proper peripheral intravenous insertion and maintenance can help prevent complications. When extravasation injury does occur, hyaluronidase may be used to help distribute the vesicant over a larger area and reduce edema, in addition to wound























































































