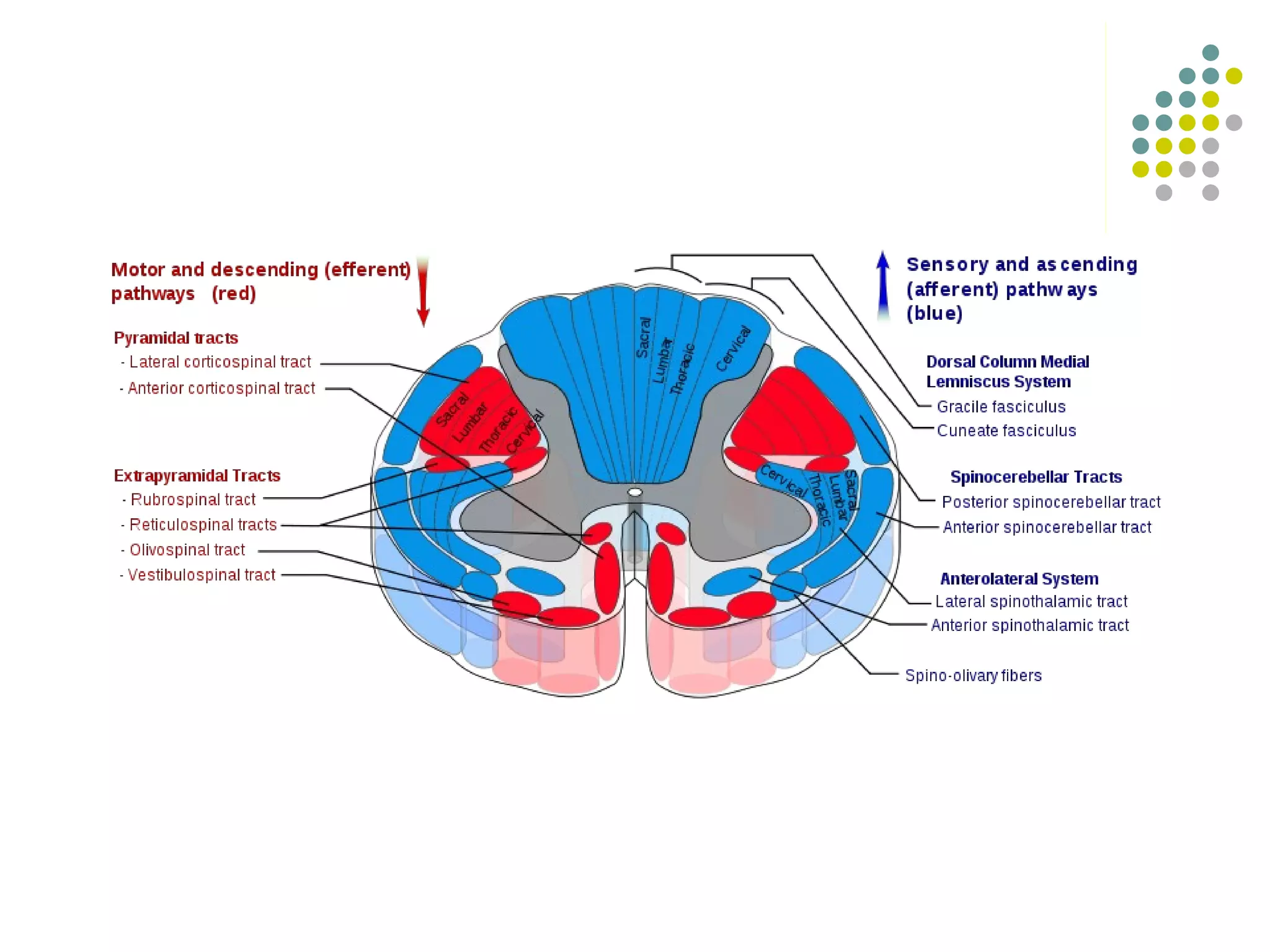
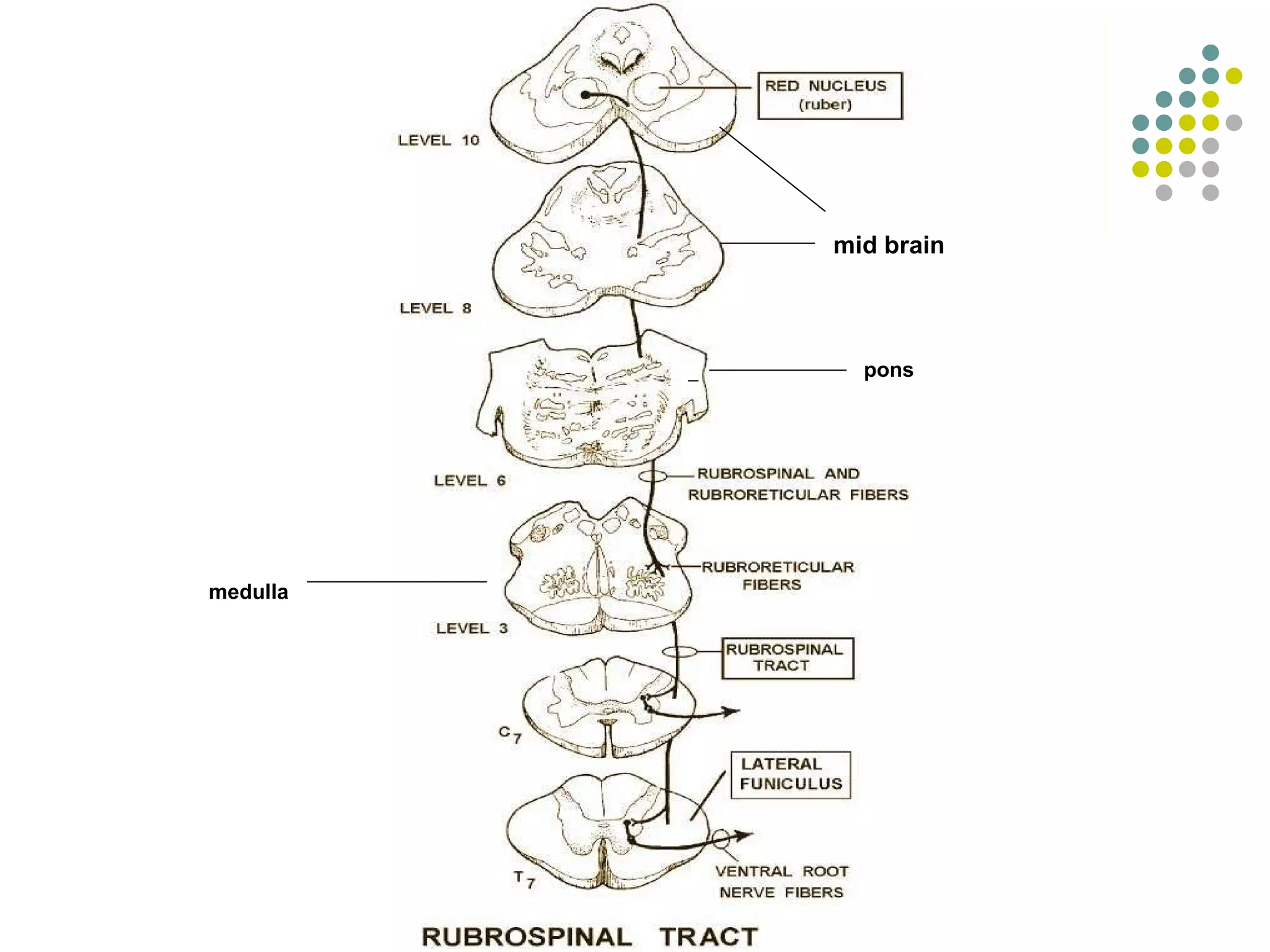
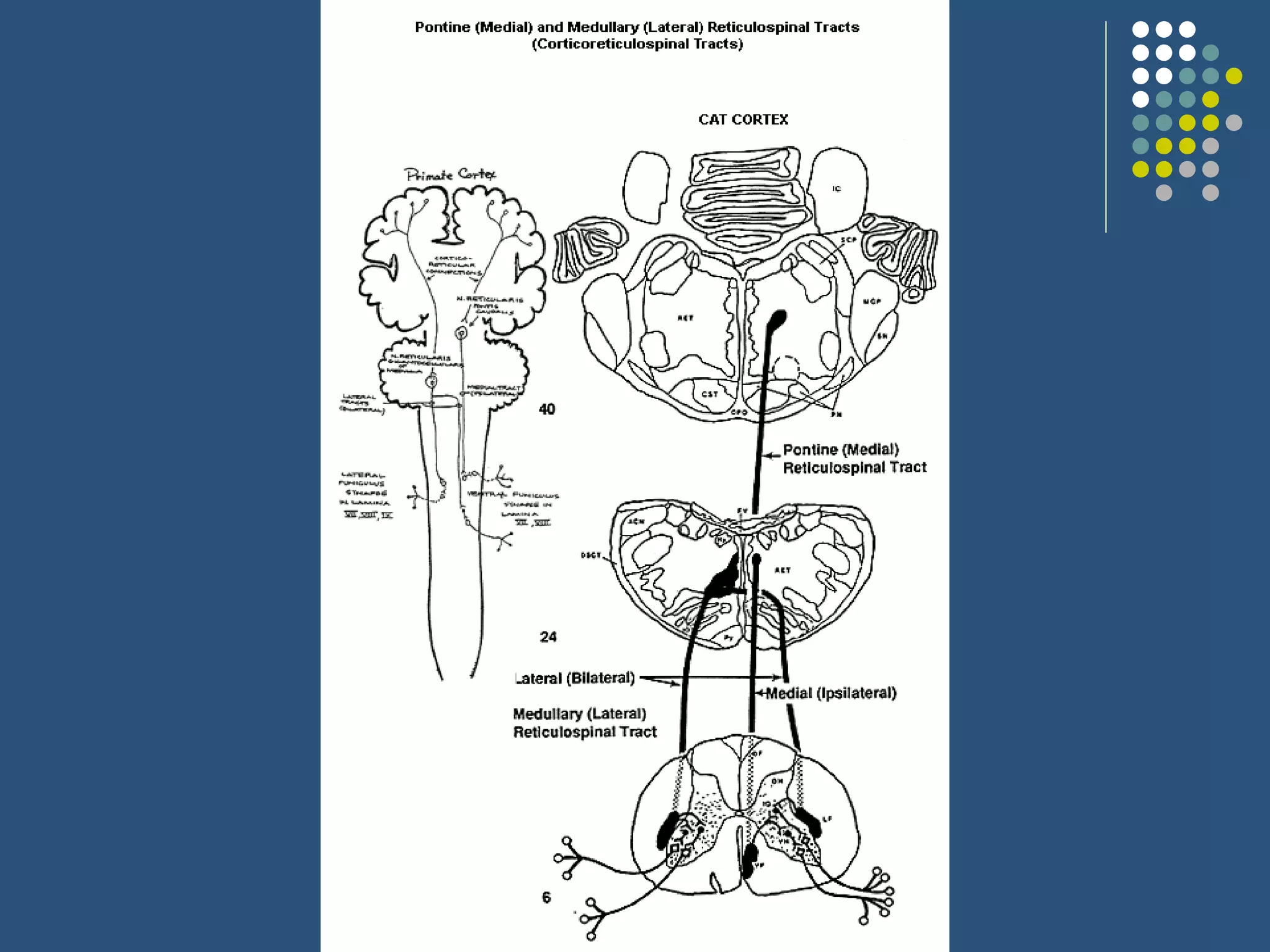
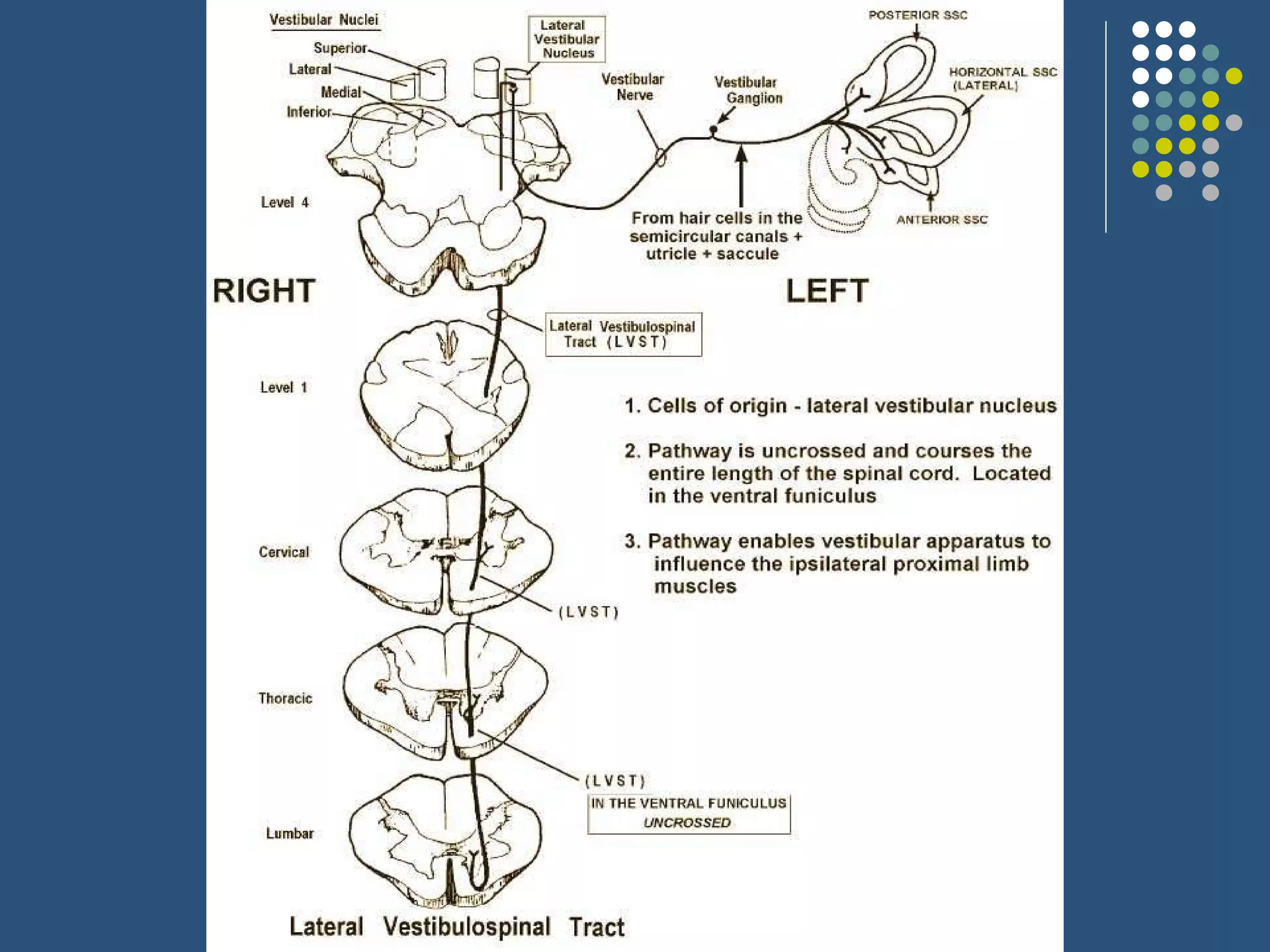
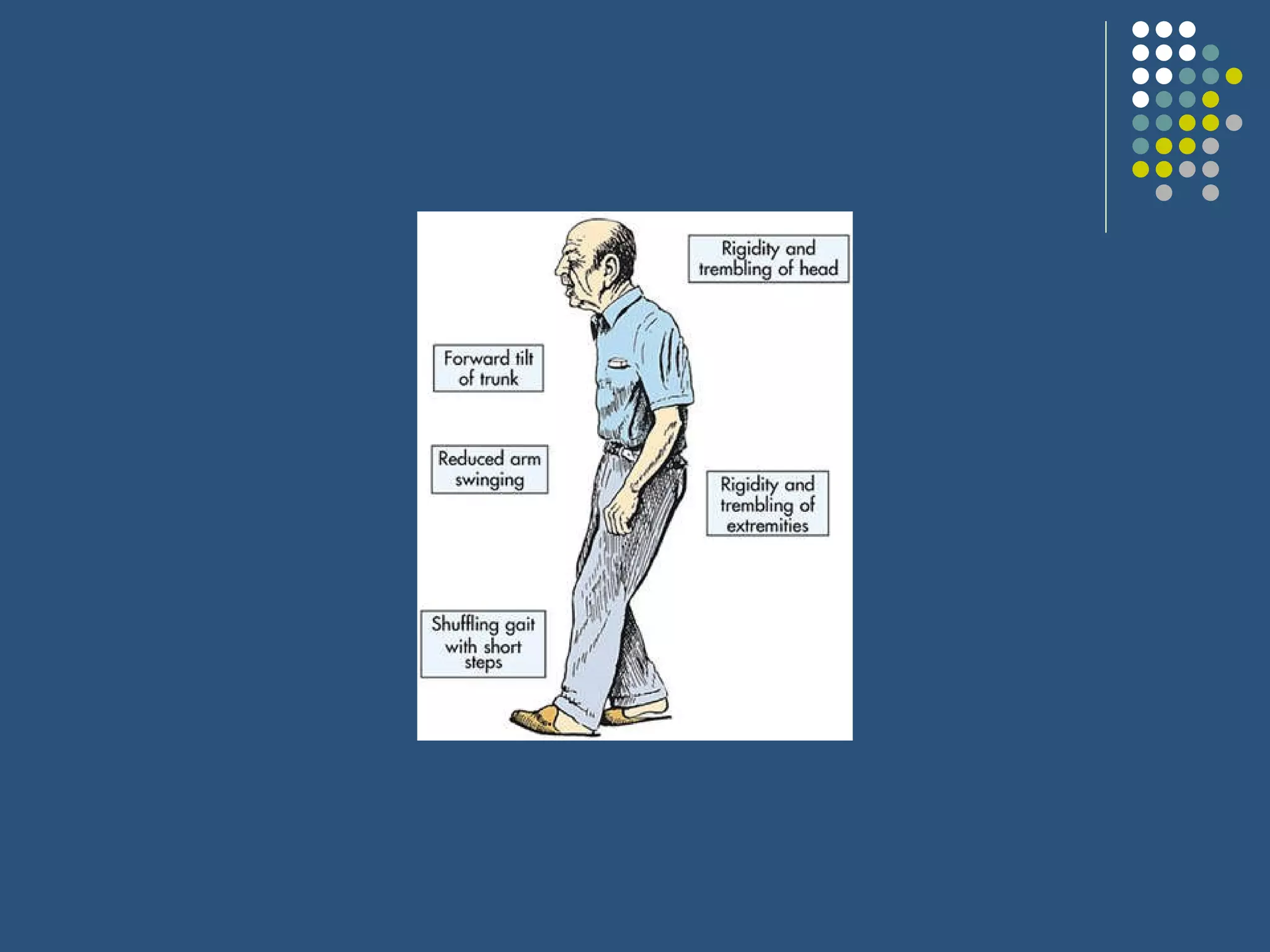
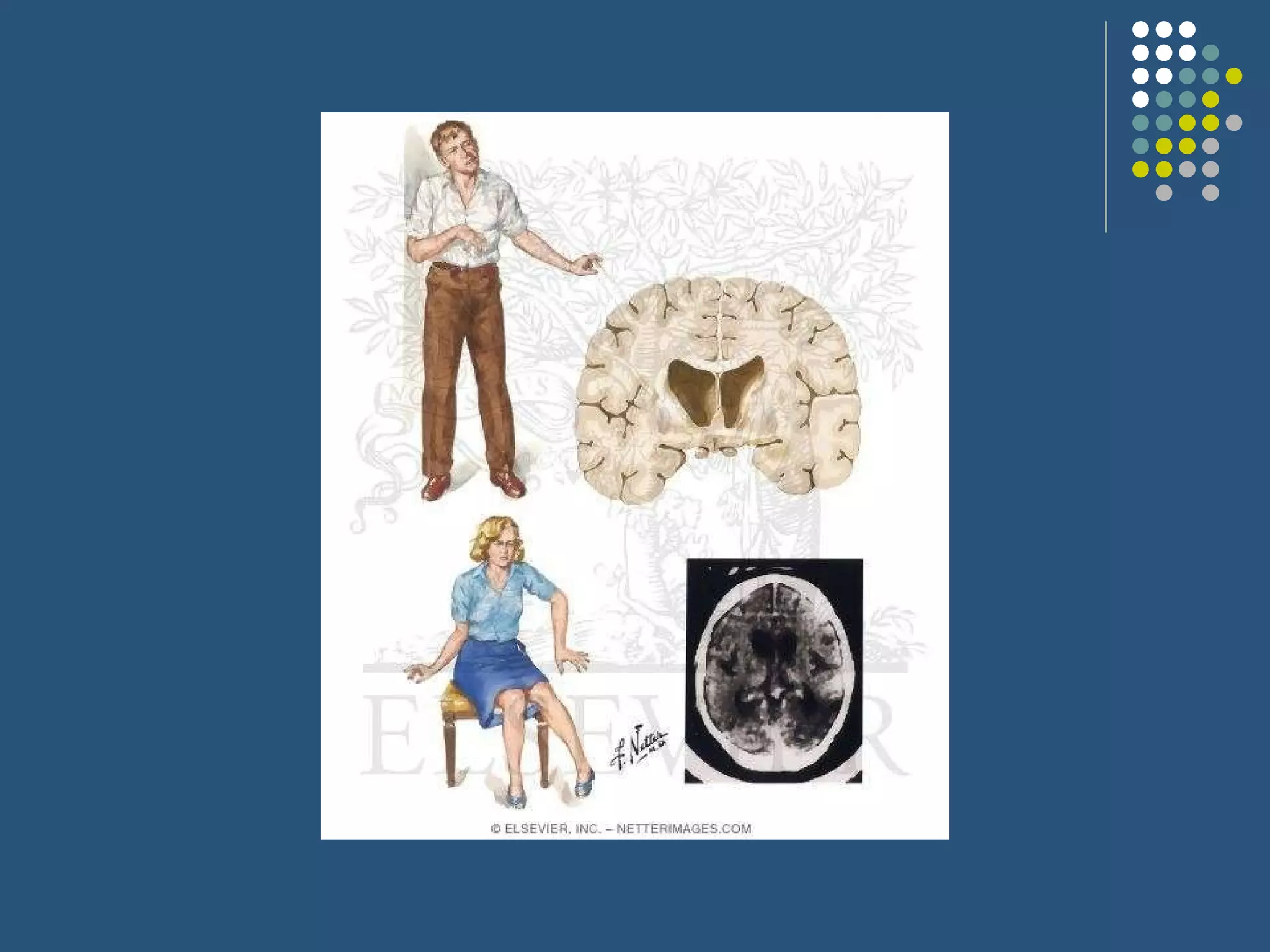
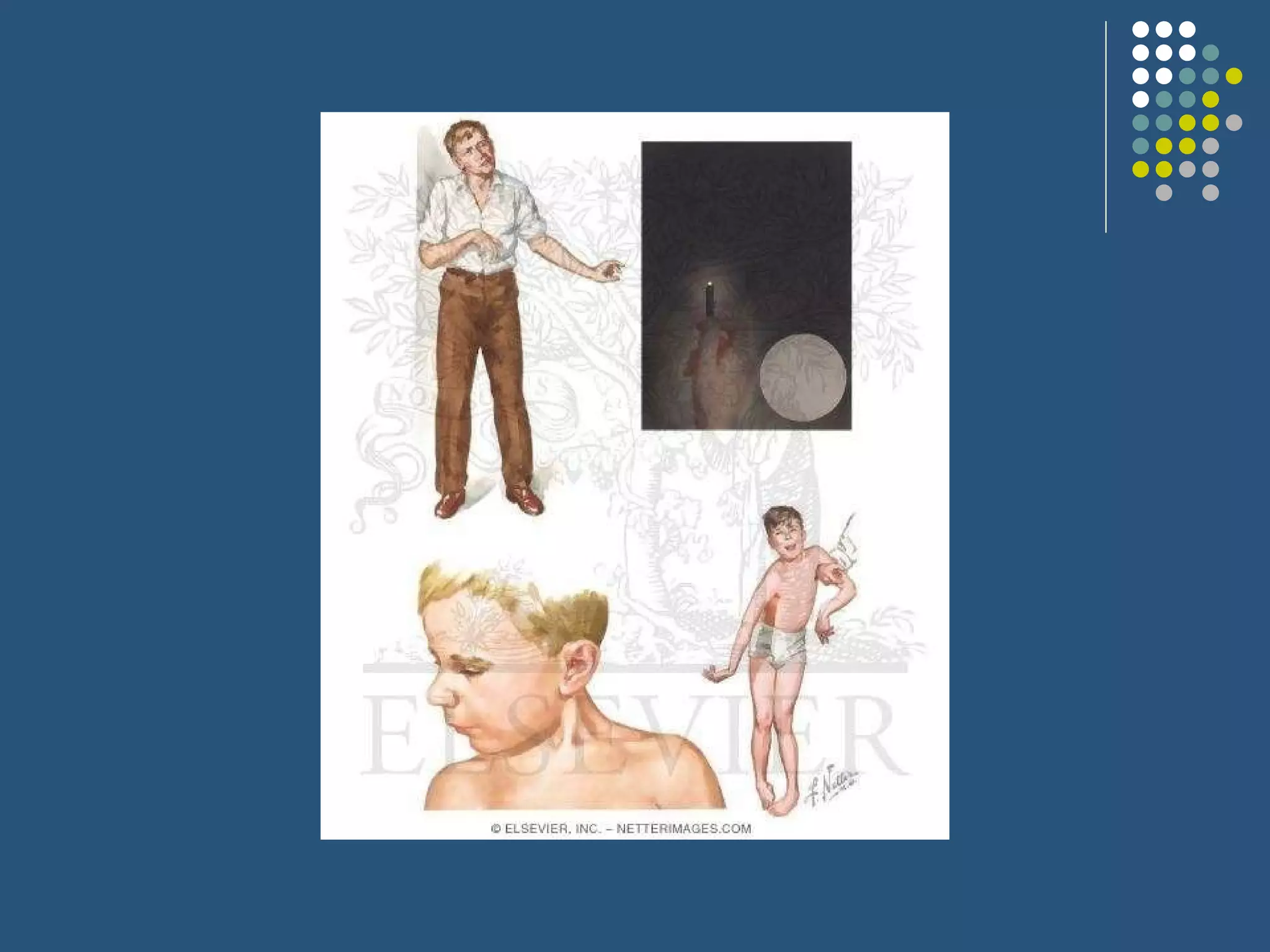
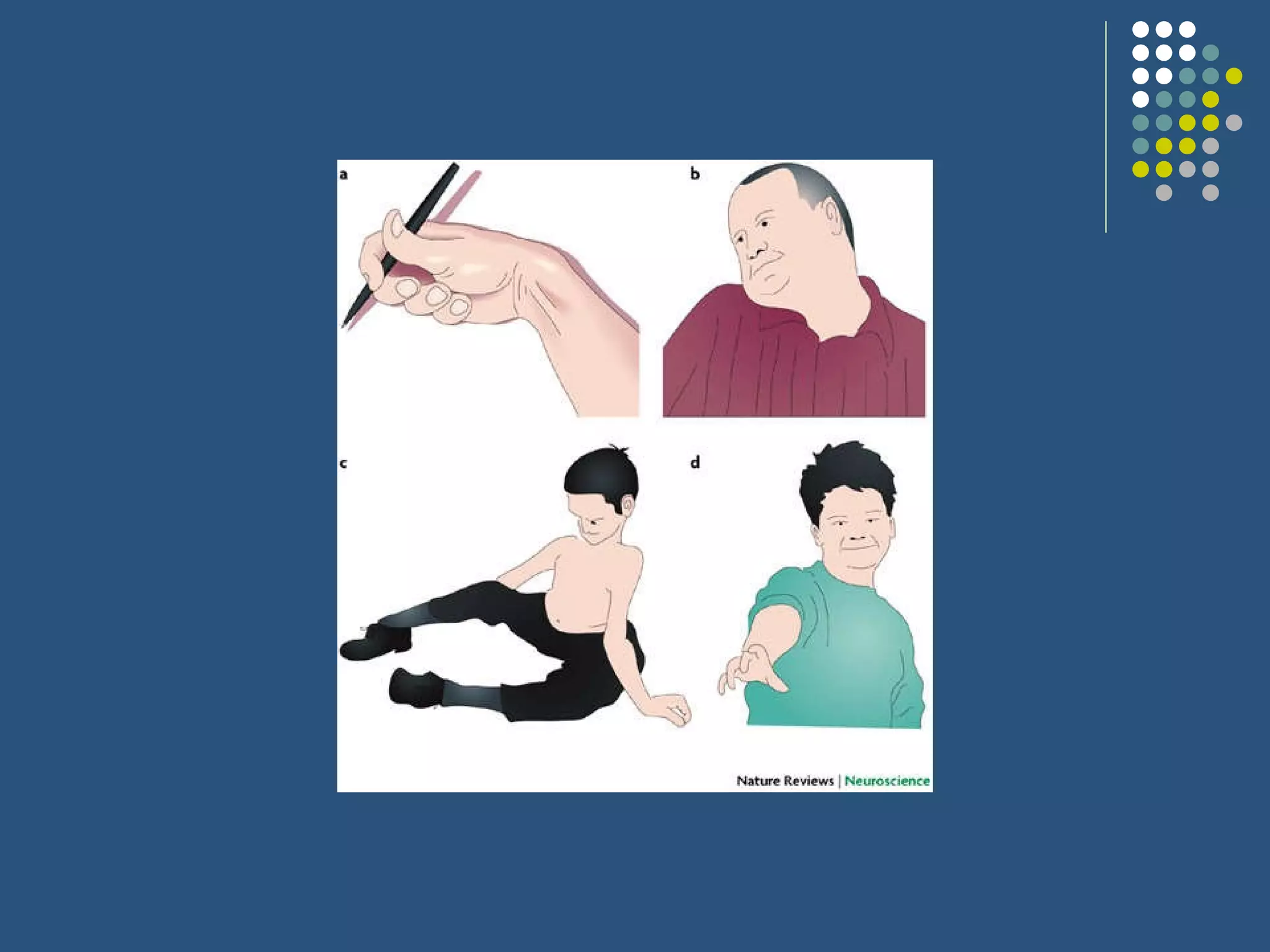
The document discusses various extrapyramidal tracts in the brain and spinal cord that help control motor function. It describes the rubrospinal, reticulospinal, olivospinal, tectospinal, and vestibulospinal tracts, including their origins, pathways, and functions. Common extrapyramidal disorders like Parkinson's disease, chorea, hemiballism, athetosis, dystonia, and tardive dyskinesia are also briefly outlined.