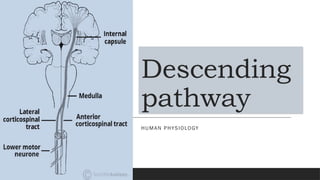
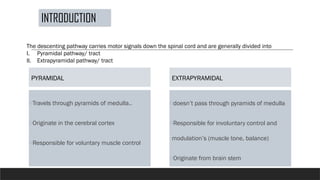
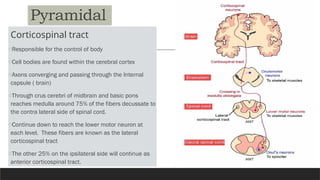
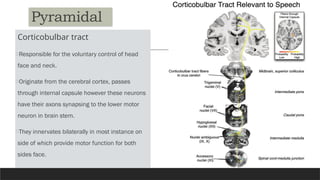
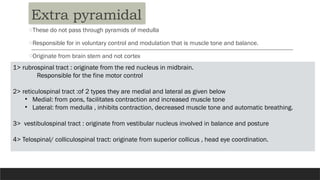
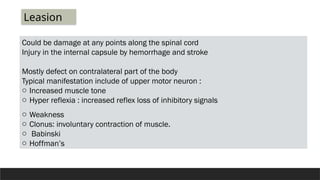
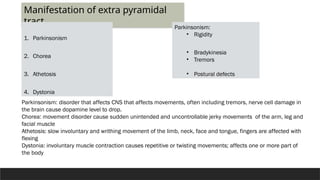
The descending pathway in human physiology carries motor signals down the spinal cord, divided into pyramidal and extrapyramidal tracts. The pyramidal tract includes the corticospinal and corticobulbar pathways, responsible for voluntary muscle control, while the extrapyramidal tract handles involuntary control and modulation. Damage to these pathways can result in various motor disorders such as parkinsonism, chorea, athetosis, and dystonia.