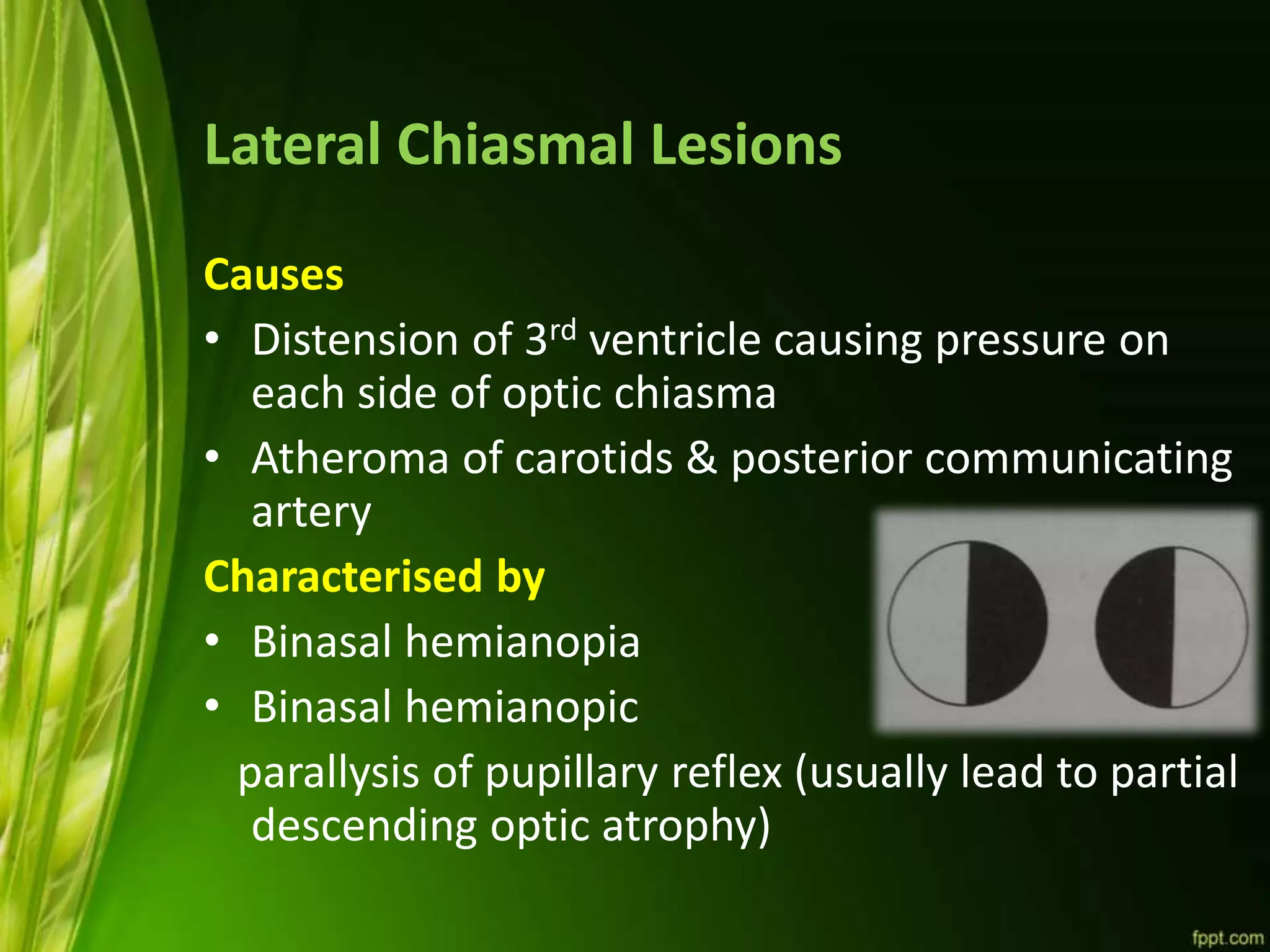
This document discusses the anatomy and variations of the optic chiasm. It describes the chiasm as a flattened structure located above the pituitary gland where the optic nerves from each eye partially cross. The temporal fibers remain uncrossed while the nasal fibers cross over. Variations in the position of the chiasm can impact which structures are involved in pituitary tumors. Lesions in the center of the chiasm cause bitemporal hemianopia while lateral lesions cause binasal hemianopia. The blood supply and relations to surrounding structures are also outlined.