

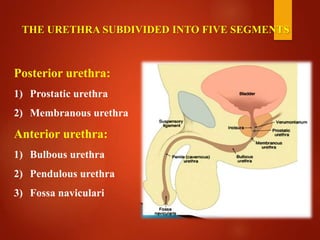
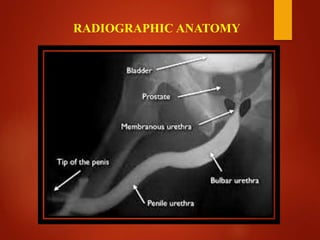







This document provides information about an opposing urethrogram procedure used to evaluate and document urethral strictures. It begins with an introduction to urethral anatomy and then describes the indications, contraindications, equipment, and technique for performing an opposing urethrogram. This involves inserting a suprapubic catheter and Foley catheter, filling the bladder with contrast medium under fluoroscopy, and obtaining images to assess any strictures present in the urethra. Potential complications are noted. The concluding sentences state that an opposing urethrogram is the only x-ray procedure that can accurately access the length of a urethral stricture.



































































