Download to read offline
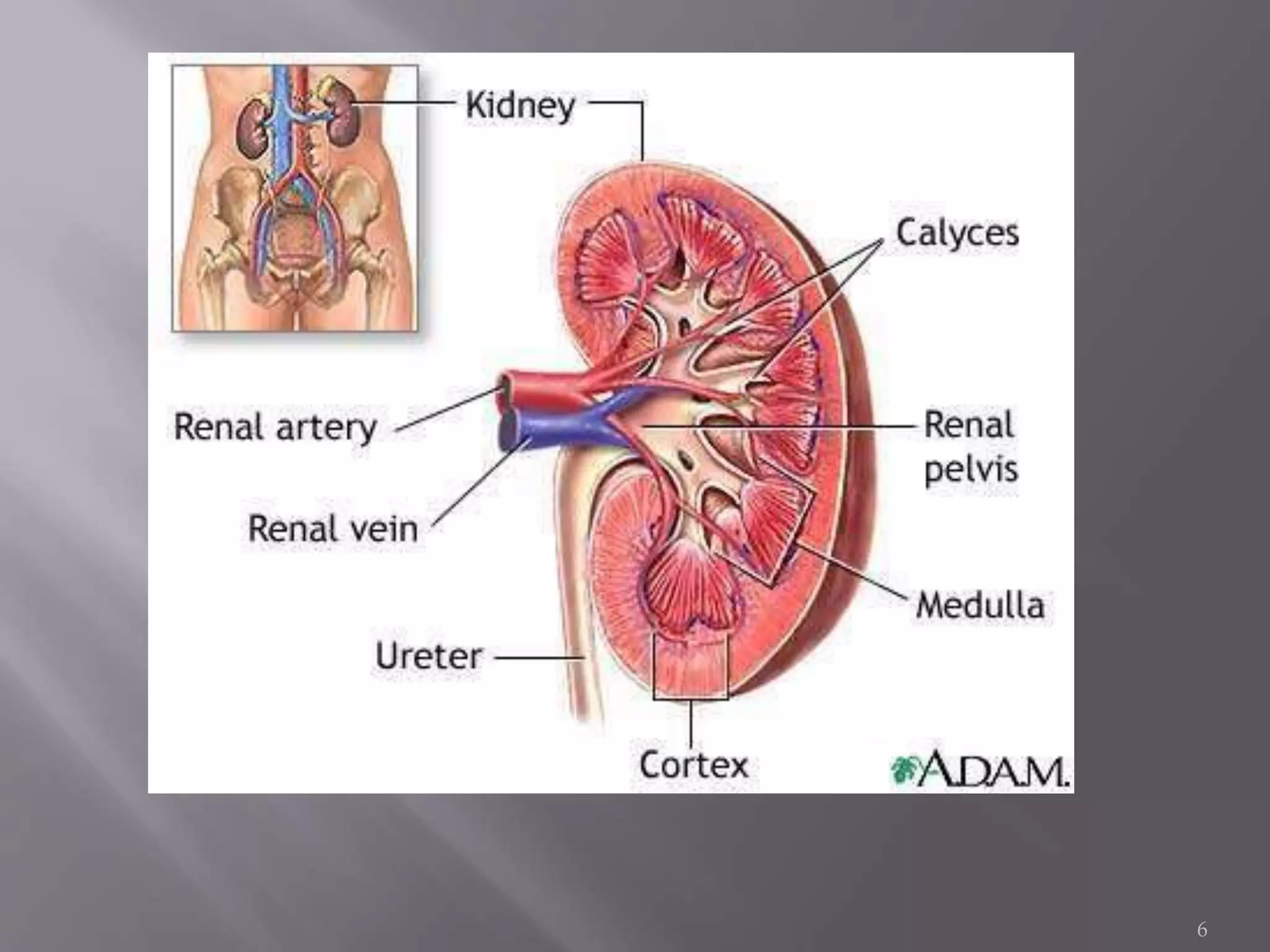
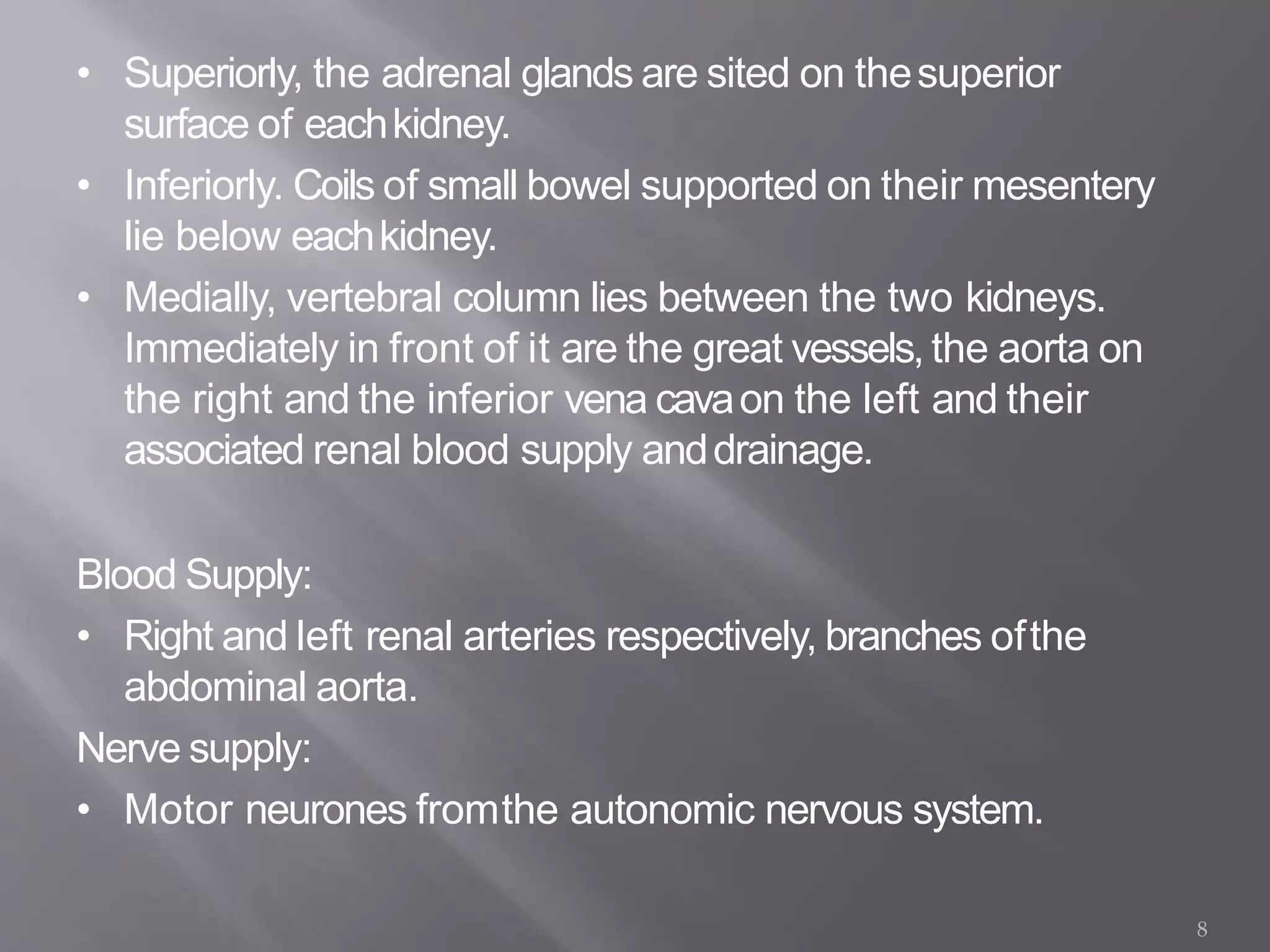
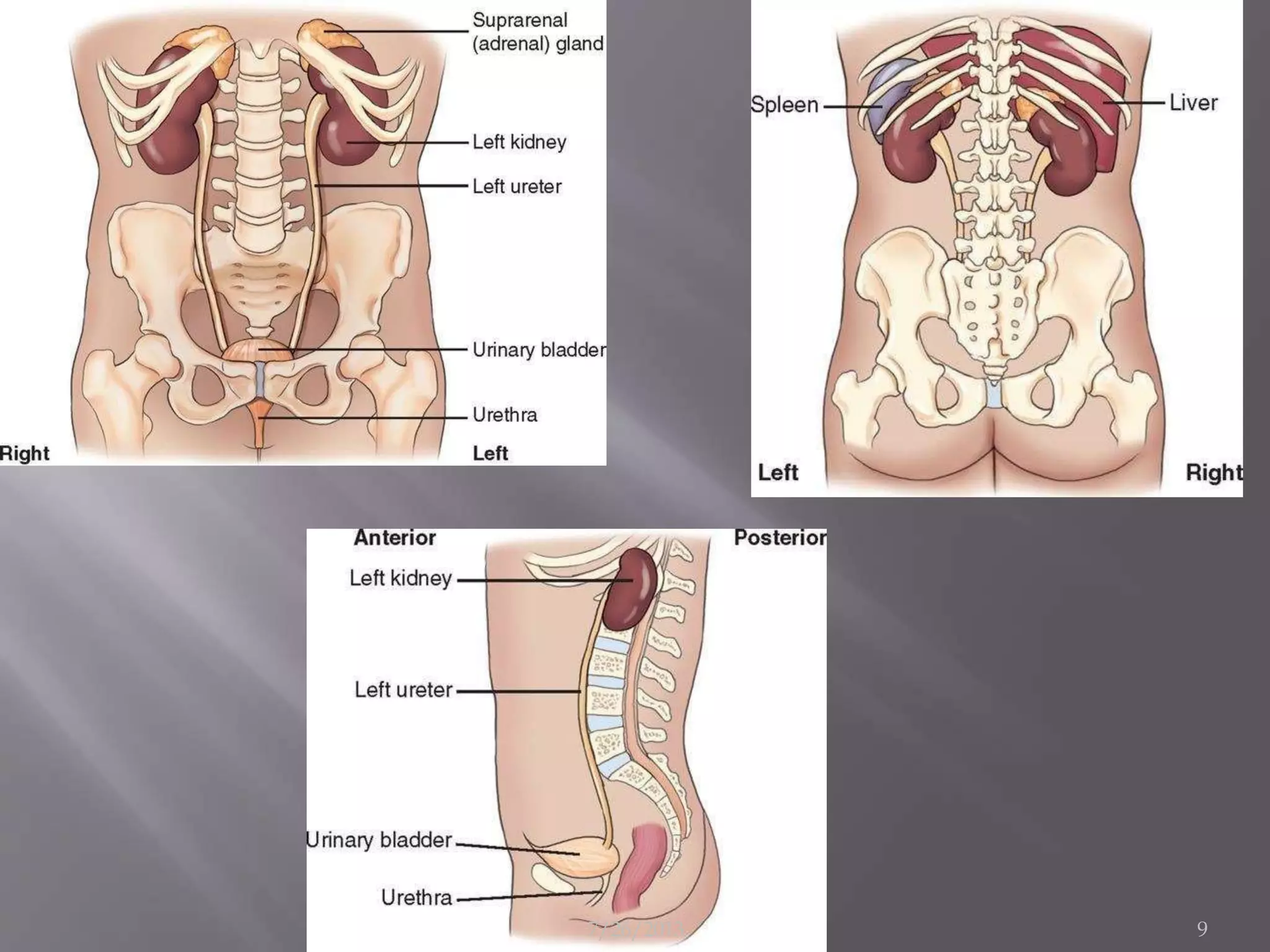
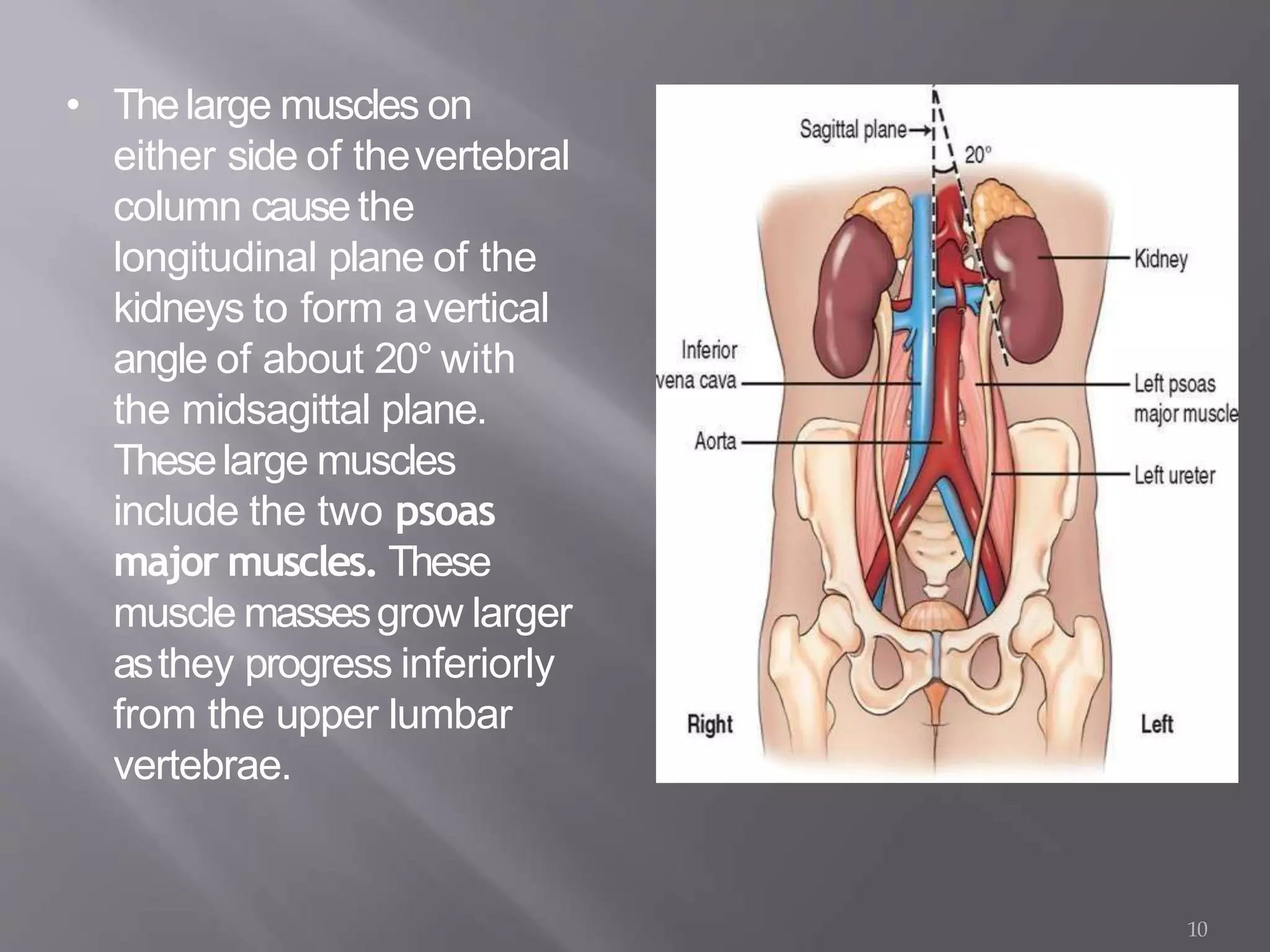



























The document discusses Intravenous Urography (IVU), a radiologic method for investigating renal drainage, particularly useful for examining upper urinary tracts. It also details the anatomy of the kidneys, ureters, and bladder, including their structures and relationships, as well as indications for the procedure and various conditions that may affect it. Additionally, it covers the technical aspects of performing IVU, patient preparation, and possible complications associated with contrast media.