Downloaded 61 times

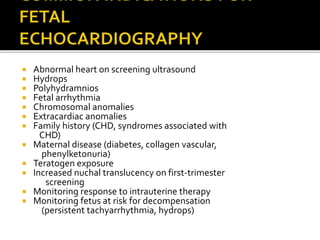
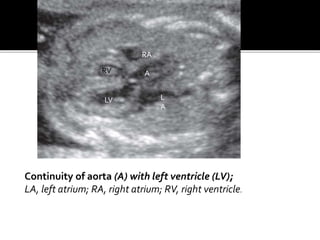
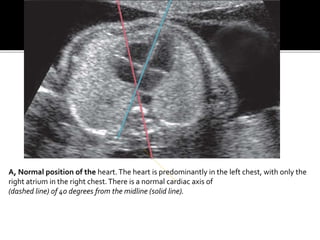


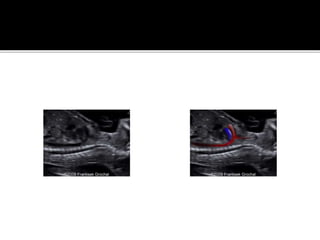
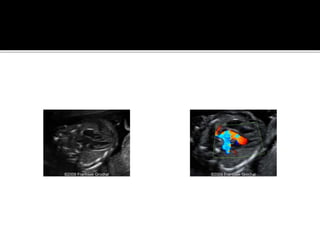
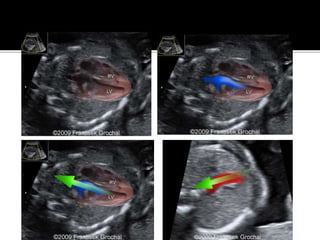
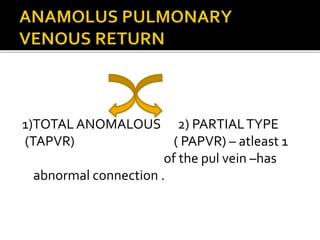


The document provides a comprehensive overview of various fetal cardiac anomalies, including their ultrasound characteristics, incidence, and associations with other conditions. It describes specific defects such as atrial septal defects, ventricular septal defects, and complex heart conditions like tetralogy of Fallot and double-outlet right ventricle. Additionally, it emphasizes the importance of ultrasound techniques in diagnosing these congenital heart diseases and their implications for fetal health.