Intermittent exotropia progresses through four phases:
1. Exophoria at distance and orthophoria at near with no symptoms
2. Intermittent exotropia at distance with orthophoria/exophoria at near and distance symptoms
3. Exotropia at distance and exophoria or intermittent exotropia at near with binocular vision near but suppression scotoma develops for distance
4. Exotropia at both distance and near with lack of binocularity
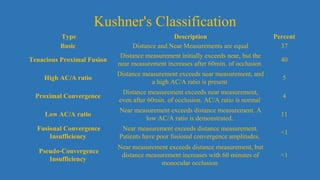
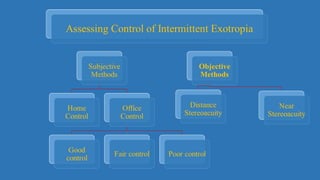
Intermittent exotropia can be classified into basic, divergence excess, convergence insufficiency, and pseudo-divergence excess types. Risk factors include positive family history,




















![Optics of contact lens and nomenclature copy [repaired] (1)](https://cdn.slidesharecdn.com/ss_thumbnails/opticsofcontactlensandnomenclature-copyrepaired1-170218054900-thumbnail.jpg?width=640&height=640&fit=bounds)


























































