Epidermoid cyst
•Download as PPT, PDF•
1 like•2,093 views

Epidermoid Cyst extended into multiple basal cisterns, internal auditory meatus, Gasser fossa & cavernous sinus.
Report
Share
Report
Share
Recommended
Trigeminal
This document summarizes key information about the trigeminal nerve including its sensory and motor distribution, lesions, and clinical presentations. It discusses supranuclear, nuclear, and peripheral lesions and their effects. Supranuclear lesions can cause pseudobulbar palsies or unilateral jaw deviation. Nuclear lesions typically involve the trigeminal nuclei and cause ipsilateral facial sensory deficits. Peripheral lesions affect the trigeminal ganglion or branches, potentially causing numbness, pain or motor deficits in the corresponding regions of the face.
9.3 the brain
The document describes the anatomy and physiology of the nervous system, including the central nervous system which is made up of the brain and spinal cord. It discusses the different parts of the brain including the cerebrum, cerebellum, pons, and medulla oblongata and their functions. The document also covers the meninges layers that surround the brain and spinal cord, cerebrospinal fluid, and the relationship between meningitis and the central nervous system.
Peripheral nerves &roots lession localisation
The document discusses the peripheral nervous system (PNS) which is divided into the somatic and autonomic nervous systems. The somatic system includes spinal nerves and cranial nerves which innervate skeletal muscles. The autonomic system regulates functions of internal organs. Some common neuropathies that can affect the PNS are discussed such as carpal tunnel syndrome, ulnar neuropathy, and polyneuropathies including Guillain-Barré syndrome. Plexopathies like brachial plexopathy and lumbosacral plexopathy are also summarized.
History & examination of edema
The document provides guidance on how to take a history and examine a patient presenting with edema. It discusses evaluating the appearance, onset, first site of appearance and associated symptoms to determine if the edema is localized or generalized. Examination of the patient should include assessing nutrition status, pallor, icterus, cyanosis, lymphadenopathy and vital signs. Demonstrating edema clinically involves applying pressure over bony prominences and looking for pitting. Specific examinations are described for cardiac, renal and ascites-related edema.
Cranial nerve syndromes
This document lists various cranial nerve syndromes, their typical causes, and locations in the brain. It describes several syndromes defined by their associated cranial nerve palsies and other neurological symptoms, as well as the lesions that usually cause each syndrome. For example, Foix syndrome involves cranial nerves 3, 4, 5 and 6 and is caused by invasive tumors of the sphenoid bone. Tolosa-Hunt syndrome affects cranial nerves 3, 4, 5 and 6 and results from aneurysms or thrombosis of the cavernous sinus.
Evaluation of brchial plexus injury
This document provides an overview of brachial plexus injury, including:
1) The anatomy of the brachial plexus is described, including its roots, trunks, divisions, cords and branches.
2) The etiology, mechanisms, and classifications of brachial plexus injuries according to Seddon and Sunderland are summarized.
3) The clinical features of brachial plexus injuries are outlined, including locations of injury, neurological examination findings, and associated deformities.
4) Common investigative tools for brachial plexus injuries like EMG, NCV, and SEP are mentioned.
Sensory disturbances at the level of thalamus and cortex
The document discusses sensory disturbances that can occur at the level of the thalamus and cortex. The thalamus acts as a sensory relay center and processes sensations before they reach the cerebral cortex. Lesions in the thalamus can cause contralateral loss of all sensations, while cortical lesions mimic thalamic lesions but only cause loss of cortical sensations. Symptoms differ depending on whether the lesion is in the thalamus or cortex.
2 brain stem akd
The document discusses the gross anatomy and internal structures of the brainstem, including the medulla, pons, and midbrain. It describes the blood supply to each region and several clinical syndromes that can result from lesions in different parts of the brainstem, such as Wallenberg syndrome from a lesion of the posterior inferior cerebellar artery affecting the medulla. It also discusses syndromes associated with lesions of the pons and midbrain, including Millard-Gubler syndrome and Weber's syndrome.
Recommended
Trigeminal
This document summarizes key information about the trigeminal nerve including its sensory and motor distribution, lesions, and clinical presentations. It discusses supranuclear, nuclear, and peripheral lesions and their effects. Supranuclear lesions can cause pseudobulbar palsies or unilateral jaw deviation. Nuclear lesions typically involve the trigeminal nuclei and cause ipsilateral facial sensory deficits. Peripheral lesions affect the trigeminal ganglion or branches, potentially causing numbness, pain or motor deficits in the corresponding regions of the face.
9.3 the brain
The document describes the anatomy and physiology of the nervous system, including the central nervous system which is made up of the brain and spinal cord. It discusses the different parts of the brain including the cerebrum, cerebellum, pons, and medulla oblongata and their functions. The document also covers the meninges layers that surround the brain and spinal cord, cerebrospinal fluid, and the relationship between meningitis and the central nervous system.
Peripheral nerves &roots lession localisation
The document discusses the peripheral nervous system (PNS) which is divided into the somatic and autonomic nervous systems. The somatic system includes spinal nerves and cranial nerves which innervate skeletal muscles. The autonomic system regulates functions of internal organs. Some common neuropathies that can affect the PNS are discussed such as carpal tunnel syndrome, ulnar neuropathy, and polyneuropathies including Guillain-Barré syndrome. Plexopathies like brachial plexopathy and lumbosacral plexopathy are also summarized.
History & examination of edema
The document provides guidance on how to take a history and examine a patient presenting with edema. It discusses evaluating the appearance, onset, first site of appearance and associated symptoms to determine if the edema is localized or generalized. Examination of the patient should include assessing nutrition status, pallor, icterus, cyanosis, lymphadenopathy and vital signs. Demonstrating edema clinically involves applying pressure over bony prominences and looking for pitting. Specific examinations are described for cardiac, renal and ascites-related edema.
Cranial nerve syndromes
This document lists various cranial nerve syndromes, their typical causes, and locations in the brain. It describes several syndromes defined by their associated cranial nerve palsies and other neurological symptoms, as well as the lesions that usually cause each syndrome. For example, Foix syndrome involves cranial nerves 3, 4, 5 and 6 and is caused by invasive tumors of the sphenoid bone. Tolosa-Hunt syndrome affects cranial nerves 3, 4, 5 and 6 and results from aneurysms or thrombosis of the cavernous sinus.
Evaluation of brchial plexus injury
This document provides an overview of brachial plexus injury, including:
1) The anatomy of the brachial plexus is described, including its roots, trunks, divisions, cords and branches.
2) The etiology, mechanisms, and classifications of brachial plexus injuries according to Seddon and Sunderland are summarized.
3) The clinical features of brachial plexus injuries are outlined, including locations of injury, neurological examination findings, and associated deformities.
4) Common investigative tools for brachial plexus injuries like EMG, NCV, and SEP are mentioned.
Sensory disturbances at the level of thalamus and cortex
The document discusses sensory disturbances that can occur at the level of the thalamus and cortex. The thalamus acts as a sensory relay center and processes sensations before they reach the cerebral cortex. Lesions in the thalamus can cause contralateral loss of all sensations, while cortical lesions mimic thalamic lesions but only cause loss of cortical sensations. Symptoms differ depending on whether the lesion is in the thalamus or cortex.
2 brain stem akd
The document discusses the gross anatomy and internal structures of the brainstem, including the medulla, pons, and midbrain. It describes the blood supply to each region and several clinical syndromes that can result from lesions in different parts of the brainstem, such as Wallenberg syndrome from a lesion of the posterior inferior cerebellar artery affecting the medulla. It also discusses syndromes associated with lesions of the pons and midbrain, including Millard-Gubler syndrome and Weber's syndrome.
Neural tube defects a case series - copy
Neural tube defects are congenital malformations that occur due to defects during neural tube formation in early embryonic development. They can be open, where neural tissue is exposed, or closed, where neural tissue is confined but covered by dysplastic skin. Ultrasound and MRI are used for prenatal diagnosis and show findings characteristic of specific defects like anencephaly, encephalocele, myelomeningocele, or craniorachischisis. Management involves prenatal counseling and postnatal surgical intervention if needed.
Brachial plexus seminar dr saumya agarwal
Brachial plexus seminar dr saumya agarwalCentral Institute of Orthopaedics, Safdarjang Hospital and VMMC, New Delhi
The brachial plexus is formed by the ventral rami of cervical and thoracic nerve roots from C5-T1. It provides motor and sensory innervation to the upper limb. Brachial plexus injuries can occur from trauma such as motorcycle accidents or obstetric injuries during childbirth. Common types of injuries include Erb's palsy affecting C5-C6 roots and Klumpke's palsy affecting C8-T1 roots. Specific nerves like the median and ulnar nerve can also be injured, resulting in paralysis of certain muscles and deformities. Evaluation involves neurological examination and special tests while management depends on the severity and nature of injury.Brain stem lessions in sensory symptoms
A 62-year-old man presented with sudden onset of unsteadiness, tendency to fall to the right side, loss of sensation in the right half of the face and left side of the torso, and dysphagia. On examination, he had partial ptosis, enophthalmos, miosis of the right eye, and cerebellar signs. Localizing the lesion based on associated neurological deficits suggests a lesion in the pons, as the patient has crossed sensory loss of the face indicative of a lower motor neuron lesion of the trigeminal nerve, as well as unilateral facial numbness and potential unilateral deafness. Lesions in specific areas of the brainstem can be localized based on the cranial nerves
Brachial plexus injury
The brachial plexus is a network of nerves that originates from the lower cervical and upper thoracic spinal nerve roots and provides motor and sensory innervation to the upper limb. It has five roots, three trunks, divisions, cords and branches. The roots emerge from the spinal nerves C5-T1. The cords are named lateral, posterior, and medial based on their relationship to the axillary artery. The plexus gives rise to many branches that innervate specific muscles and skin areas of the upper limb. Variations commonly occur in the formation of the lateral cord. Injuries can happen at the level of the roots, cords or branches and cause different functional deficits depending on the location and extent of injury
Eye
The document describes the anatomy and structures of the eye. It discusses the three layers (tunics) that make up the eye - the outer fibrous layer, middle vascular layer, and inner retinal layer. It describes key optical components such as the cornea, pupil, iris, lens, vitreous humor, and aqueous humor. The document also outlines production and flow of aqueous humor, the six extrinsic eye muscles, and provides diagrams of eye anatomy including layers and muscles.
Brachial plexus
This document discusses the electrophysiological evaluation of the brachial plexus using nerve conduction studies and electromyography. It describes the anatomy of the brachial plexus including its roots, trunks, divisions, cords, and terminal nerves. It explains how to assess each element of the brachial plexus using sensory nerve action potentials, compound muscle action potentials, and electromyography findings. It also discusses the patterns seen with different types of brachial plexus lesions and provides guidance on timing of electrodiagnostic testing and prognostication.
Anatomy and embryology of anterior chamber angle ppt new
This document discusses the anatomy and embryology of the angle of the anterior chamber. It begins by defining the angle of the anterior chamber as the recess formed between the posterior surface of the cornea and anterior surface of the iris, which is the main pathway for drainage of aqueous humor. It then covers the embryology of eye development from the formation of the optic vesicle and stalk to the optic cup. The document also discusses conditions that affect the angle such as congenital glaucoma and posterior embryotoxon. Assessment techniques for the anterior chamber angle including gonioscopy, torchlight examination, and imaging modalities like UBM and OCT are provided.
Cerebellum
This document provides an overview of the cerebellum. It discusses the gross anatomy, radiographic appearance, development, functional divisions, blood supply, and common pathologies of the cerebellum. Key points covered include the connections between the cerebellum and brainstem, the cortical layers and circuitry, the phylogenetic and functional roles of different cerebellar regions, and common causes of cerebellar ataxia including vascular, infectious, autoimmune, metabolic, neoplastic and inherited etiologies. Diagrams are provided to illustrate cerebellar anatomy and examples of various cerebellar lesions.
Brachial Plexus Injury
The brachial plexus is formed from nerve roots exiting the cervical and thoracic spinal cord. It can be injured through trauma, tumors, or birth injuries. A brachial plexus injury causes weakness, numbness, pain and deformities in the arm and hand. Physical examination tests specific muscles innervated by different nerve roots to localize the level of injury. Imaging studies and electrodiagnostic tests help evaluate the severity and location of injury to guide treatment.
Radiological anatomy of the brain
The document describes the anatomy and development of the brain. It discusses that the brain begins as a single-celled zygote that divides and forms into three germ layers. Thickening in the ectoderm forms the neural plate which folds to become the neural tube, dividing into the brain and spinal cord. The brain consists of the cerebrum, brainstem, and cerebellum. Various imaging modalities can be used to image the detailed structures and anatomy of the brain.
Congenital malformation of cns
The document discusses various congenital malformations of the central nervous system (CNS), including neural tube defects and cortical migrational anomalies. It describes specific conditions like anencephaly, encephalocele, spina bifida, lissencephaly, polymicrogyria, heterotopia, and focal cortical dysplasia. It provides ICD-10 codes for different CNS malformations and includes images to illustrate various normal and abnormal brain structures.
Seminar on clinical aspects of stroke
This document provides an overview of ischemic stroke and related anatomy. It defines cerebral ischemic stroke as acute focal neurological dysfunction caused by focal brain infarction. It discusses transient ischemic attacks and different types of strokes, including ischemic and hemorrhagic. The document then reviews the anatomy related to ischemic strokes, including the arterial supply of the brain and the circle of Willis. It describes the clinical features and symptoms associated with occlusions or infarctions in different vascular territories, such as the internal carotid, anterior cerebral, middle cerebral, and posterior cerebral arteries. Finally, it notes that while clinical exams can help localize strokes, imaging is important to detect small or multiple infarctions.
Brainstem stroke syndromes
1. Medial medullary syndrome results from lesions of the corticospinal tract, medial lemniscus, and hypoglossal nucleus, causing contralateral hemiparesis, loss of trunk/extremity sensation, and ipsilateral tongue paralysis respectively.
2. Lateral medullary syndrome results from lesions affecting structures like the vestibular nuclei, inferior cerebellar peduncle and vagal nuclei, causing nystagmus, ipsilateral cerebellar signs, and laryngeal/pharyngeal paralysis.
3. Pontine syndromes include medial inferior pontine syndrome affecting corticospinal and medial lemniscus tracts and lateral inferior pontine syndrome affecting
Radiology 5th year, 1st & 2nd lectures (Dr. Ameer)
Skull and brain imaging techniques such as CT and MRI are standard for investigating trauma, while ultrasound angiography is limited to detecting stenosis, aneurysms, and arteriovenous malformations. CT is useful for detecting fractures, edema, contusions, hemorrhages, and other abnormalities. MRI provides additional information on lesions and is more accurate for diagnosing conditions such as multiple sclerosis and arteriovenous malformations. Various imaging findings help characterize common brain pathologies including tumors, infarcts, hemorrhages, and infections.
Cerebellum clinical
This document provides information about the cerebellum and cerebellar disorders. It discusses examination of ataxia, symptoms of cerebellar ataxia including limb ataxia, truncal ataxia, dysarthria, and visual symptoms. It also covers different types of cerebellar disorders like tumors, infections, metabolic disorders, and case scenarios of patients presenting with ataxia. Imaging findings are described that can help identify the cause of ataxia.
Cerebellar degeneration
Cerebellar degeneration is the degeneration of nerves in the cerebellum, the part of the brain that controls balance and muscle coordination. Symptoms include impaired balance, unsteady walking, tremors, and slurred speech. It can be caused by head trauma, stroke, tumors, infections like chickenpox, or autoimmune diseases like multiple sclerosis. The diagnosis involves testing balance, reflexes, coordination and other functions controlled by the cerebellum. Treatment depends on the underlying cause but may include surgery, antibiotics, medications to reduce inflammation, or blood thinners.
Nerve block
The document describes various nerve blocks for the upper and lower extremities, including the elbow, wrist, digits, ankle, and toes. Nerve blocks of the femoral nerve and three-in-one block are also covered. Additionally, the document discusses nerve blocks for the head and face, such as inferior alveolar, mental, greater occipital, and lesser occipital nerve blocks. Locations and techniques for administering each nerve block are illustrated with diagrams.
CRiedinger_blood_supply_brain
The document summarizes the major arteries that supply the brain and spinal cord, including the anterior cerebral artery (ACA), middle cerebral artery (MCA), posterior cerebral artery (PCA), superior cerebellar artery (SCA), anterior inferior cerebellar artery (AICA), posterior inferior cerebellar artery (PICA), anterior spinal artery, and posterior spinal artery. It details the origin, course, and territory supplied by each artery.
Basics of Neuroradiology
Basics of Neuroradiology
Neuroradiology is an essential tool in management of patients with neurological and neurosurgical disorders. The aim of this presentation will be to acquaint the reader to understand how images are formed on a computed tomography (CT) and magnetic resonance imaging (MRI) along with a review of the relevant neuroanatomy. This understanding will be helpful to the reader in interpretation of images and diagnosis of various neurological disorders.
Brain stem syndromes
The document discusses various syndromes associated with lesions in different areas of the brainstem. It describes syndromes related to lesions of the posterior cerebral artery including Dejerine-Roussy syndrome and Claude's syndrome. It also summarizes syndromes caused by lesions in specific areas of the pons including the basis pontis, ventral pons, dorsal pons, and ventral medial pons. Syndromes involving the medulla are also outlined such as Wallenberg's lateral medullary syndrome and medial medullary syndrome. Finally, it provides an overview of the anatomy and blood supply of the midbrain and medulla.
Dermoid & Epidermoid Cysts
This document discusses dermoid and epidermoid cysts. Dermoid cysts can occur in various locations including near the eyes, nose, chin, and chest. Midline dermoids often require CT or MRI before surgery as intracranial extension is found in about 36% of cases. Sebaceous or epidermoid cysts contain fatty secretions and are commonly found on the scalp or face, though they do not originate from sebaceous glands.
Epidermoid Cyst
This document describes epidermoid cysts, which are the most common orbital neoplasms in children. They result from ectodermal tissue becoming embedded in bone sutures during development. Epidermoid cysts typically appear as soft, slowly enlarging masses near the superotemporal orbital margin. While usually painless, they can cause cosmetic issues or symptoms like proptosis and diplopia if large or located internally. The document then reports a case study of a 5-year-old girl with an epidermoid cyst that was surgically excised. Histopathology confirmed the diagnosis of an epidermoid cyst.
More Related Content
What's hot
Neural tube defects a case series - copy
Neural tube defects are congenital malformations that occur due to defects during neural tube formation in early embryonic development. They can be open, where neural tissue is exposed, or closed, where neural tissue is confined but covered by dysplastic skin. Ultrasound and MRI are used for prenatal diagnosis and show findings characteristic of specific defects like anencephaly, encephalocele, myelomeningocele, or craniorachischisis. Management involves prenatal counseling and postnatal surgical intervention if needed.
Brachial plexus seminar dr saumya agarwal
Brachial plexus seminar dr saumya agarwalCentral Institute of Orthopaedics, Safdarjang Hospital and VMMC, New Delhi
The brachial plexus is formed by the ventral rami of cervical and thoracic nerve roots from C5-T1. It provides motor and sensory innervation to the upper limb. Brachial plexus injuries can occur from trauma such as motorcycle accidents or obstetric injuries during childbirth. Common types of injuries include Erb's palsy affecting C5-C6 roots and Klumpke's palsy affecting C8-T1 roots. Specific nerves like the median and ulnar nerve can also be injured, resulting in paralysis of certain muscles and deformities. Evaluation involves neurological examination and special tests while management depends on the severity and nature of injury.Brain stem lessions in sensory symptoms
A 62-year-old man presented with sudden onset of unsteadiness, tendency to fall to the right side, loss of sensation in the right half of the face and left side of the torso, and dysphagia. On examination, he had partial ptosis, enophthalmos, miosis of the right eye, and cerebellar signs. Localizing the lesion based on associated neurological deficits suggests a lesion in the pons, as the patient has crossed sensory loss of the face indicative of a lower motor neuron lesion of the trigeminal nerve, as well as unilateral facial numbness and potential unilateral deafness. Lesions in specific areas of the brainstem can be localized based on the cranial nerves
Brachial plexus injury
The brachial plexus is a network of nerves that originates from the lower cervical and upper thoracic spinal nerve roots and provides motor and sensory innervation to the upper limb. It has five roots, three trunks, divisions, cords and branches. The roots emerge from the spinal nerves C5-T1. The cords are named lateral, posterior, and medial based on their relationship to the axillary artery. The plexus gives rise to many branches that innervate specific muscles and skin areas of the upper limb. Variations commonly occur in the formation of the lateral cord. Injuries can happen at the level of the roots, cords or branches and cause different functional deficits depending on the location and extent of injury
Eye
The document describes the anatomy and structures of the eye. It discusses the three layers (tunics) that make up the eye - the outer fibrous layer, middle vascular layer, and inner retinal layer. It describes key optical components such as the cornea, pupil, iris, lens, vitreous humor, and aqueous humor. The document also outlines production and flow of aqueous humor, the six extrinsic eye muscles, and provides diagrams of eye anatomy including layers and muscles.
Brachial plexus
This document discusses the electrophysiological evaluation of the brachial plexus using nerve conduction studies and electromyography. It describes the anatomy of the brachial plexus including its roots, trunks, divisions, cords, and terminal nerves. It explains how to assess each element of the brachial plexus using sensory nerve action potentials, compound muscle action potentials, and electromyography findings. It also discusses the patterns seen with different types of brachial plexus lesions and provides guidance on timing of electrodiagnostic testing and prognostication.
Anatomy and embryology of anterior chamber angle ppt new
This document discusses the anatomy and embryology of the angle of the anterior chamber. It begins by defining the angle of the anterior chamber as the recess formed between the posterior surface of the cornea and anterior surface of the iris, which is the main pathway for drainage of aqueous humor. It then covers the embryology of eye development from the formation of the optic vesicle and stalk to the optic cup. The document also discusses conditions that affect the angle such as congenital glaucoma and posterior embryotoxon. Assessment techniques for the anterior chamber angle including gonioscopy, torchlight examination, and imaging modalities like UBM and OCT are provided.
Cerebellum
This document provides an overview of the cerebellum. It discusses the gross anatomy, radiographic appearance, development, functional divisions, blood supply, and common pathologies of the cerebellum. Key points covered include the connections between the cerebellum and brainstem, the cortical layers and circuitry, the phylogenetic and functional roles of different cerebellar regions, and common causes of cerebellar ataxia including vascular, infectious, autoimmune, metabolic, neoplastic and inherited etiologies. Diagrams are provided to illustrate cerebellar anatomy and examples of various cerebellar lesions.
Brachial Plexus Injury
The brachial plexus is formed from nerve roots exiting the cervical and thoracic spinal cord. It can be injured through trauma, tumors, or birth injuries. A brachial plexus injury causes weakness, numbness, pain and deformities in the arm and hand. Physical examination tests specific muscles innervated by different nerve roots to localize the level of injury. Imaging studies and electrodiagnostic tests help evaluate the severity and location of injury to guide treatment.
Radiological anatomy of the brain
The document describes the anatomy and development of the brain. It discusses that the brain begins as a single-celled zygote that divides and forms into three germ layers. Thickening in the ectoderm forms the neural plate which folds to become the neural tube, dividing into the brain and spinal cord. The brain consists of the cerebrum, brainstem, and cerebellum. Various imaging modalities can be used to image the detailed structures and anatomy of the brain.
Congenital malformation of cns
The document discusses various congenital malformations of the central nervous system (CNS), including neural tube defects and cortical migrational anomalies. It describes specific conditions like anencephaly, encephalocele, spina bifida, lissencephaly, polymicrogyria, heterotopia, and focal cortical dysplasia. It provides ICD-10 codes for different CNS malformations and includes images to illustrate various normal and abnormal brain structures.
Seminar on clinical aspects of stroke
This document provides an overview of ischemic stroke and related anatomy. It defines cerebral ischemic stroke as acute focal neurological dysfunction caused by focal brain infarction. It discusses transient ischemic attacks and different types of strokes, including ischemic and hemorrhagic. The document then reviews the anatomy related to ischemic strokes, including the arterial supply of the brain and the circle of Willis. It describes the clinical features and symptoms associated with occlusions or infarctions in different vascular territories, such as the internal carotid, anterior cerebral, middle cerebral, and posterior cerebral arteries. Finally, it notes that while clinical exams can help localize strokes, imaging is important to detect small or multiple infarctions.
Brainstem stroke syndromes
1. Medial medullary syndrome results from lesions of the corticospinal tract, medial lemniscus, and hypoglossal nucleus, causing contralateral hemiparesis, loss of trunk/extremity sensation, and ipsilateral tongue paralysis respectively.
2. Lateral medullary syndrome results from lesions affecting structures like the vestibular nuclei, inferior cerebellar peduncle and vagal nuclei, causing nystagmus, ipsilateral cerebellar signs, and laryngeal/pharyngeal paralysis.
3. Pontine syndromes include medial inferior pontine syndrome affecting corticospinal and medial lemniscus tracts and lateral inferior pontine syndrome affecting
Radiology 5th year, 1st & 2nd lectures (Dr. Ameer)
Skull and brain imaging techniques such as CT and MRI are standard for investigating trauma, while ultrasound angiography is limited to detecting stenosis, aneurysms, and arteriovenous malformations. CT is useful for detecting fractures, edema, contusions, hemorrhages, and other abnormalities. MRI provides additional information on lesions and is more accurate for diagnosing conditions such as multiple sclerosis and arteriovenous malformations. Various imaging findings help characterize common brain pathologies including tumors, infarcts, hemorrhages, and infections.
Cerebellum clinical
This document provides information about the cerebellum and cerebellar disorders. It discusses examination of ataxia, symptoms of cerebellar ataxia including limb ataxia, truncal ataxia, dysarthria, and visual symptoms. It also covers different types of cerebellar disorders like tumors, infections, metabolic disorders, and case scenarios of patients presenting with ataxia. Imaging findings are described that can help identify the cause of ataxia.
Cerebellar degeneration
Cerebellar degeneration is the degeneration of nerves in the cerebellum, the part of the brain that controls balance and muscle coordination. Symptoms include impaired balance, unsteady walking, tremors, and slurred speech. It can be caused by head trauma, stroke, tumors, infections like chickenpox, or autoimmune diseases like multiple sclerosis. The diagnosis involves testing balance, reflexes, coordination and other functions controlled by the cerebellum. Treatment depends on the underlying cause but may include surgery, antibiotics, medications to reduce inflammation, or blood thinners.
Nerve block
The document describes various nerve blocks for the upper and lower extremities, including the elbow, wrist, digits, ankle, and toes. Nerve blocks of the femoral nerve and three-in-one block are also covered. Additionally, the document discusses nerve blocks for the head and face, such as inferior alveolar, mental, greater occipital, and lesser occipital nerve blocks. Locations and techniques for administering each nerve block are illustrated with diagrams.
CRiedinger_blood_supply_brain
The document summarizes the major arteries that supply the brain and spinal cord, including the anterior cerebral artery (ACA), middle cerebral artery (MCA), posterior cerebral artery (PCA), superior cerebellar artery (SCA), anterior inferior cerebellar artery (AICA), posterior inferior cerebellar artery (PICA), anterior spinal artery, and posterior spinal artery. It details the origin, course, and territory supplied by each artery.
Basics of Neuroradiology
Basics of Neuroradiology
Neuroradiology is an essential tool in management of patients with neurological and neurosurgical disorders. The aim of this presentation will be to acquaint the reader to understand how images are formed on a computed tomography (CT) and magnetic resonance imaging (MRI) along with a review of the relevant neuroanatomy. This understanding will be helpful to the reader in interpretation of images and diagnosis of various neurological disorders.
Brain stem syndromes
The document discusses various syndromes associated with lesions in different areas of the brainstem. It describes syndromes related to lesions of the posterior cerebral artery including Dejerine-Roussy syndrome and Claude's syndrome. It also summarizes syndromes caused by lesions in specific areas of the pons including the basis pontis, ventral pons, dorsal pons, and ventral medial pons. Syndromes involving the medulla are also outlined such as Wallenberg's lateral medullary syndrome and medial medullary syndrome. Finally, it provides an overview of the anatomy and blood supply of the midbrain and medulla.
What's hot (20)
Anatomy and embryology of anterior chamber angle ppt new
Anatomy and embryology of anterior chamber angle ppt new
Radiology 5th year, 1st & 2nd lectures (Dr. Ameer)
Radiology 5th year, 1st & 2nd lectures (Dr. Ameer)
Viewers also liked
Dermoid & Epidermoid Cysts
This document discusses dermoid and epidermoid cysts. Dermoid cysts can occur in various locations including near the eyes, nose, chin, and chest. Midline dermoids often require CT or MRI before surgery as intracranial extension is found in about 36% of cases. Sebaceous or epidermoid cysts contain fatty secretions and are commonly found on the scalp or face, though they do not originate from sebaceous glands.
Epidermoid Cyst
This document describes epidermoid cysts, which are the most common orbital neoplasms in children. They result from ectodermal tissue becoming embedded in bone sutures during development. Epidermoid cysts typically appear as soft, slowly enlarging masses near the superotemporal orbital margin. While usually painless, they can cause cosmetic issues or symptoms like proptosis and diplopia if large or located internally. The document then reports a case study of a 5-year-old girl with an epidermoid cyst that was surgically excised. Histopathology confirmed the diagnosis of an epidermoid cyst.
Dermoid Cyst
This document summarizes and differentiates between various types of cysts: dermoid cysts, which are lined with squamous epithelium; teratomatous cysts; sequestration cysts; implantation cysts; branchial cysts in the neck; cystic hygromas in the neck; sebaceous cysts; sinuses and fistulas. It notes the locations, patient demographics, clinical features, diagnostic tools, and treatments for each type of cyst.
Dermoid cyst
Dermoid cysts are cysts lined with squamous epithelium that contain skin adnexa such as sweat glands, sebaceous glands, and hair follicles. There are several types of dermoid cysts including congenital dermoid cysts that form along embryonic fusion lines and can cause bony defects, implantation dermoid cysts that form after skin implantation injuries, and teratomatous dermoid cysts containing tissues from all germ layers. Dermoid cysts typically present as slow-growing, painless swellings and are diagnosed based on location and imaging findings showing cystic masses sometimes eroding adjacent bone. Excision is the treatment.
IMAGING OF INTRACRANIAL PRIMARY NON-NEOPLASTIC CYSTS
- Cysts are common brain imaging findings that can be difficult to differentiate based on imaging alone. A location-based approach is helpful for establishing a differential diagnosis.
- Common non-neoplastic, non-infectious cysts include choroid plexus cysts, arachnoid cysts, pineal cysts, and enlarged perivascular (Virchow-Robin) spaces. These cysts have characteristic imaging appearances that can help distinguish them from one another.
- Differentiating cysts may require assessing features such as location within the brain, signal characteristics, enhancement patterns, and associated imaging findings. This location-based algorithm aids in narrowing the diagnostic possibilities.
Haemangioma , lymphangioma and dermoid cyst
This document provides information on haemangioma, lymphangioma, and dermoid cyst. It discusses:
- The different types of haemangioma (capillary, cavernous, plexiform) and examples like salmon patches, port-wine stains, and strawberry angiomas.
- Lymphangiomas are malformations of the lymphatic system that can be capillary or cavernous (cystic hygroma).
- Dermoid cysts are lined by squamous epithelium and contain mixtures of cells/tissues. There are different types like sequestration, implantation, teratomatous, and tubulodermoid cysts.
- It provides
Cervical Rib
A cervical rib is an extra rib that arises from the seventh cervical vertebra. It occurs in 0.6-0.8% of the population. Cervical ribs usually do not cause symptoms but can potentially lead to thoracic outlet syndrome by compressing nerves. This occurs when the cervical rib and scalene muscles compress the lower trunk of the brachial plexus or subclavian artery. Symptoms include pain, numbness, and weakness in the arm and hand. Diagnosis involves identifying nerve compression during physical exam maneuvers. Surgery to remove the cervical rib and divide scalene muscles may be required if neurological symptoms develop. Physiotherapy focuses on reducing pain, maintaining range of motion and muscle strength, and
THORACIC OUTLET SYNDROM (TOS)
Thoracic outlet syndrome (TOS) occurs when the blood vessels or nerves in the thoracic outlet area between the neck and armpit are compressed. The thoracic outlet contains several narrow spaces through which the nerves and vessels pass. Physical therapy is the primary treatment for TOS and aims to open the spaces and correct shoulder positioning. Surgery to remove part of the first rib may be considered if physical therapy fails or for complications involving blood vessels or nerves. Proper diagnosis involves patient examination maneuvers to reproduce symptoms and imaging tests to identify anatomical abnormalities.
Cutaneous Cysts
Cysts with a lining of stratified squamous epithelium: Epidermoid cyst
Milium
Trichilemmal cyst
Vellus hair cyst
Steatocystoma
Dermoid cyst
Cysts lined with non-stratified squamous epithelium: Hidrocystoma, Eccrine or Apocrine
Cysts without an epithelial lining: Mucocele
Digital mucous cyst
Ganglion
Thoracic outlet syndrome
Thoracic outlet syndrome is caused by compression of the neurovascular bundle in the thoracic outlet. It can occur in the interscalene triangle, costoclavicular space, or subcoracoid area. Symptoms include pain, numbness, and weakness in the arm. Diagnosis involves physical exam maneuvers like Adson's test and imaging. Treatment begins with posture correction and physical therapy; surgery to remove the first rib or cervical rib may be needed for persistent or progressive symptoms.
Thoracic outlet syndrome
Thoracic outlet syndrome (TOS) refers to compression of the neurovascular structures in the thoracic outlet. There are two main types - neurogenic and vascular. Neurogenic TOS is more common and involves compression of the brachial plexus nerves, while vascular TOS involves compression of the subclavian artery or vein. Symptoms vary depending on the affected structure but may include pain, numbness, cold intolerance, or vascular symptoms like swelling. Diagnosis involves physical exam maneuvers and imaging tests like ultrasound or MRI. Treatment begins with conservative measures like stretching and strengthening, but refractory cases may require injections or surgeries like scalenectomy to decompress the area.
thoracic outlet syndrome
This document provides information on thoracic outlet syndrome (TOS). It begins with a brief history and defines TOS as abnormal compression of the neurovascular bundle in the thoracic outlet. It describes the relevant anatomy and compartments of the thoracic outlet. The document discusses the causes, types, symptoms, and diagnostic approaches for the neurogenic, venous, and arterial forms of TOS. It provides details on conservative and surgical treatment options.
Diagnostic Imaging of Cerebellopontine Angle Masses
This document provides an overview of cerebellopontine angle masses, including their incidence, location, and radiographic features. It discusses the most common masses such as vestibular schwannoma (acoustic neuroma), CPA meningioma, and epidermoid cyst. For each type of mass, it describes their typical appearance on CT and MRI scans, including signal characteristics and enhancement patterns. It also provides differential diagnoses to help distinguish between different pathologies that can present in the CPA region. The goal is to help readers learn as much as possible about CPA masses to aid in successful diagnosis and management.
Radiological imaging of intracranial cystic lesions
This document provides information on intracranial cystic lesions, including their classification, etiology, imaging appearance and characteristics. It discusses both neoplastic and non-neoplastic cysts, as well as infectious and congenital cysts. Specific cysts covered include arachnoid cysts, dermoid cysts, epidermoid cysts and neuroglial cysts. For each type of cyst, the document provides details on location, appearance on CT, MRI, differential diagnosis and treatment.
Viewers also liked (14)
IMAGING OF INTRACRANIAL PRIMARY NON-NEOPLASTIC CYSTS
IMAGING OF INTRACRANIAL PRIMARY NON-NEOPLASTIC CYSTS
Diagnostic Imaging of Cerebellopontine Angle Masses
Diagnostic Imaging of Cerebellopontine Angle Masses
Radiological imaging of intracranial cystic lesions
Radiological imaging of intracranial cystic lesions
More from Ruth Martín Boizas
Right varicocele. Ultrasound.
The medical document discusses three findings: a right varicocele, dilated veins within the right testis; rette testis dilatation, enlarged veins within the network of veins draining the testis; and an epididymal cyst, a fluid-filled sac within the epididymis, the coiled tubular structure that collects and transports sperm from the testis.
2nd meningiomas meet up
O documento discute vários casos de pacientes que sofreram recidivas de meningiomas ou desenvolveram múltiplos meningiomas. Detalha tratamentos como cirurgia e embolização para remover os tumores e controlar o crescimento de novos tumores. Também menciona um caso raro de múltipla meningiomatose.
Type 3 Frontal Cell
The document discusses two anatomical structures: Type 3 Frontal Cell and Agger nasi. Type 3 Frontal Cell refers to a specific type of frontal sinus cell located in the frontal bone above the nose. Agger nasi refers to a small bony projection located in the nasal cavity near the front of the nasal septum.
Hypoglossal Nerve Schwannoma
A patient presented with a hypoglossal nerve schwannoma located in the cisternal segment that was imaged with various MRI sequences including 3D CISS, T1 TSE, FLAIR, VIBE, post-gadolinium SPACE, and post-gadolinium to characterize the tumor and its relationship to surrounding structures.
Congenital Cholesteatoma of the Mastoid Bone on CT& MRI
Congenital cholesteatoma of the mastoid bone is a rare, non-epithelial cyst or tumor that exists in the mastoid bone at birth. Computed tomography (CT) and magnetic resonance imaging (MRI) are useful in evaluating congenital cholesteatoma and can help determine the extent of involvement of the mastoid bone and surrounding structures. Surgical removal is usually required to prevent complications like bone erosion and hearing loss.
Mantle B-Cell Lymphoma: Extradural & Foraminal Relapse
A patient was experiencing a relapse of mantle B-cell lymphoma that had spread outside the spinal cord into the extradural space and spinal foramina. Magnetic resonance imaging (MRI) and positron emission tomography-computed tomography (PET-CT) scans using fat saturated and non-fat saturated post-gadolinium T1 spin echo sequences were performed to evaluate the extent of the relapse.
Epilepsy in Preterm Neonate MRI
Epilepsy in Preterm Neonate MRI (2D TOF MIP, 3D MPRAGE, Diffusion, BLADE FLAIR; T1 TSE, TSTIR, T2 TSE & Tractography) . Temporary Cytotoxic Edema. Third Day of
Life. Total Recovery 2 weeks later.
Intracavernous Arachnoid Cyst MRI
An arachnoid cyst is a fluid-filled sac that develops within the arachnoid membrane layers that surround the brain or spinal cord. Magnetic resonance imaging (MRI) is often used to diagnose arachnoid cysts as it can clearly visualize the size, location, and other characteristics of the cyst. MRI is a useful non-invasive tool to evaluate arachnoid cysts and help determine if any treatment may be needed.
Choroidal Angioma on Image
Color doppler Ultrasound, PET-CT and MRI (TSTIR, Diffusion, pre & postcontrast T1 SE & T2 GE) to differentiate from Melanoma.
Virchow-Robin versus Lacunar Infarct CT & MRI
This document discusses the differences between a lacunar infarct and a Virchow-Robin space as seen on CT and MRI scans. A lacunar infarct is typically larger than 5mm, asymmetric, located in the superior two-thirds of the putamen, and not isointense with CSF. In contrast, a Virchow-Robin space is usually less than 5mm, symmetric, located in the inferior third of the putamen, and isointense with CSF. While these are the general differences, the document notes there was an asymmetric case that was unusual.
Alzheimer’s Disease Image Findings
Alzheimer's disease causes brain atrophy that can be seen on imaging tests. It initially affects the hippocampus and entorhinal cortex, then spreads to the posterior cingulum, medial temporal lobe, and insular cortex. Over time, atrophy progresses to the prefrontal and orbitofrontal cortices bilaterally in a symmetric and diffuse pattern.
Mild cognitive Impairment & Dementia MRI Protocol
I have decided to use this MRI protocol to study patients with clinical suspicion of Mild Cognitive Impairment & Dementia.
1.2 mm isotropic sagittal T1 3D MP-RAGE is centered on thalamus to be used for Voxel Based Morphometry, if necessary.
Axial T2 GE is used to discover small blood foci secondary to amyloid angiopathy.
DTI is used for VOIs on previously determined strategic areas to try to diagnose the type of dementia by image findings.
Voxel-Based Morphometry in Alzheimer's Disease 1
Example 1: Global Neuronal Volume Loss. Hipocampal, Entorhinal, Central & Postcentral Selective Neuronal Loss.
Ecchordosis Physaliphora
Ecchordosis Physaliphora. Cystic Clival Lesion. Notochord Remnant. CT & MRI.
Petrous Apex Mucocele
CT & MRI of Left Petrous Apex Mucocele. Sequences on MRI: CISS 3D, SE T1, B600 & ADC. Expansion to Carotid Canal & Posterior Fossa.
Giant Fusiform Medial Cerebral Artery Aneurysm
49 years old woman that comes to E.R. with Midriais & Comatous State. Routine Brain CT shows Subrachnoid Hemorrhage. Willis angioCT MIP & VR depicts Giant Fusiform MCA Aneurysm.
Multiple System Atrophy Cerebellar type
MRI of an 80 years old woman with piramidalism. Middle Cerebellar Peduncles & Anterior Pons Atrophy. Dp-T2 TSE, FLAIR & ADC Hyperintense Putaminal Ribbon. Decrease Naa/Cr & Cho/Cr ratios in pons & middle cerebellar peduncles on H1 MRS.
Pulmonary Embolism CT
I.V. Contrast CT. Pulmonary Embolism. 10 b Branch. Multicoloured Volume Rendering.
Surgicel MRI 2
Surgicel is a bioabsorbable topical haemostatic agent used to control bleeding in surgical procedures. How to differentiate its signal from Haemoglobin degradation products?
Note: There was an interpretative mistake first time uploaded: Blood signal was misinterpreted. I upload the correction. Sorry!.
Spinal tuberculous leptomeningitis & subdural empyema & lately intraspinal tu...
A patient presented with spinal tuberculous leptomeningitis and subdural empyema as seen on MRI, with leptomeningeal enhancement and lung cavitated nodules. The patient underwent posterior laminectomy for the spinal condition. Follow up MRIs one month and three weeks later showed progression of the leptomeningeal nodular enhancement and a new subdural empyema, indicating active intraspinal tuberculosis despite surgery.
More from Ruth Martín Boizas (20)
Congenital Cholesteatoma of the Mastoid Bone on CT& MRI
Congenital Cholesteatoma of the Mastoid Bone on CT& MRI
Mantle B-Cell Lymphoma: Extradural & Foraminal Relapse
Mantle B-Cell Lymphoma: Extradural & Foraminal Relapse
Spinal tuberculous leptomeningitis & subdural empyema & lately intraspinal tu...
Spinal tuberculous leptomeningitis & subdural empyema & lately intraspinal tu...
Recently uploaded
Nano-gold for Cancer Therapy chemistry investigatory project
chemistry investigatory project
The development of nanogold-based cancer therapy could revolutionize oncology by providing a more targeted, less invasive treatment option. This project contributes to the growing body of research aimed at harnessing nanotechnology for medical applications, paving the way for future clinical trials and potential commercial applications.
Cancer remains one of the leading causes of death worldwide, prompting the need for innovative treatment methods. Nanotechnology offers promising new approaches, including the use of gold nanoparticles (nanogold) for targeted cancer therapy. Nanogold particles possess unique physical and chemical properties that make them suitable for drug delivery, imaging, and photothermal therapy.
Cervical Disc Arthroplasty ORSI 2024.pptx
Indication and installation of a mobile cervical disc prosthesis. Benefits of the PRODISC C VIVO mobile disc prosthesis (Centinel Spine)
acne vulgaris -Mpharm (2nd semester) Cosmetics and cosmeceuticals
cosmetics and cosmeceuticals
Muskan
mpharm
2nd semester
Guru Gobind Singh college of pharmacy, yamunanagar, haryana
Helminthiasis or Worm infestation in Children for Nursing students
Brief description worm infestation/Helminthiasis for Basic B.Sc Nursing students
Call Girls In Mumbai +91-7426014248 High Profile Call Girl Mumbai
Call Girls In Mumbai +91-7426014248 High Profile Call Girl Mumbai
Demystifying Fallopian Tube Blockage- Grading the Differences and Implication...
Fallopian tube blockage may cause female infertility. For treatment, herbal medicine Fuyan Pill can be a solution.
Medical Quiz ( Online Quiz for API Meet 2024 ).pdf
This quiz was conducted as a promotional event for the 2024 Annual Meet of Kerala Chapter of API.
More than 20 participants took part everyday !
NARCOTICS- POLICY AND PROCEDURES FOR ITS USE
This document outlines policies and procedures for handling narcotic and controlled drugs in NABH accredited hospitals.
Skin Diseases That Happen During Summer.
Summer is a time for fun in the sun, but the heat and humidity can also wreak havoc on your skin. From itchy rashes to unwanted pigmentation, several skin conditions become more prevalent during these warmer months.
Breast cancer: Post menopausal endocrine therapy
Breast cancer in postmenopausal women with hormone receptor-positive (HR+) status is a common and complex condition that necessitates a multifaceted approach to management. HR+ breast cancer means that the cancer cells grow in response to hormones such as estrogen and progesterone. This subtype is prevalent among postmenopausal women and typically exhibits a more indolent course compared to other forms of breast cancer, which allows for a variety of treatment options.
Diagnosis and Staging
The diagnosis of HR+ breast cancer begins with clinical evaluation, imaging, and biopsy. Imaging modalities such as mammography, ultrasound, and MRI help in assessing the extent of the disease. Histopathological examination and immunohistochemical staining of the biopsy sample confirm the diagnosis and hormone receptor status by identifying the presence of estrogen receptors (ER) and progesterone receptors (PR) on the tumor cells.
Staging involves determining the size of the tumor (T), the involvement of regional lymph nodes (N), and the presence of distant metastasis (M). The American Joint Committee on Cancer (AJCC) staging system is commonly used. Accurate staging is critical as it guides treatment decisions.
Treatment Options
Endocrine Therapy
Endocrine therapy is the cornerstone of treatment for HR+ breast cancer in postmenopausal women. The primary goal is to reduce the levels of estrogen or block its effects on cancer cells. Commonly used agents include:
Selective Estrogen Receptor Modulators (SERMs): Tamoxifen is a SERM that binds to estrogen receptors, blocking estrogen from stimulating breast cancer cells. It is effective but may have side effects such as increased risk of endometrial cancer and thromboembolic events.
Aromatase Inhibitors (AIs): These drugs, including anastrozole, letrozole, and exemestane, lower estrogen levels by inhibiting the aromatase enzyme, which converts androgens to estrogen in peripheral tissues. AIs are generally preferred in postmenopausal women due to their efficacy and safety profile compared to tamoxifen.
Selective Estrogen Receptor Downregulators (SERDs): Fulvestrant is a SERD that degrades estrogen receptors and is used in cases where resistance to other endocrine therapies develops.
Combination Therapies
Combining endocrine therapy with other treatments enhances efficacy. Examples include:
Endocrine Therapy with CDK4/6 Inhibitors: Palbociclib, ribociclib, and abemaciclib are CDK4/6 inhibitors that, when combined with endocrine therapy, significantly improve progression-free survival in advanced HR+ breast cancer.
Endocrine Therapy with mTOR Inhibitors: Everolimus, an mTOR inhibitor, can be added to endocrine therapy for patients who have developed resistance to aromatase inhibitors.
Chemotherapy
Chemotherapy is generally reserved for patients with high-risk features, such as large tumor size, high-grade histology, or extensive lymph node involvement. Regimens often include anthracyclines and taxanes.
Osvaldo Bernardo Muchanga-GASTROINTESTINAL INFECTIONS AND GASTRITIS-2024.pdf
Osvaldo Bernardo Muchanga-GASTROINTESTINAL INFECTIONS AND GASTRITIS-2024.pdfOsvaldo Bernardo Muchanga
GASTROINTESTINAL INFECTIONS AND GASTRITIS
Osvaldo Bernardo Muchanga
Gastrointestinal Infections
GASTROINTESTINAL INFECTIONS result from the ingestion of pathogens that cause infections at the level of this tract, generally being transmitted by food, water and hands contaminated by microorganisms such as E. coli, Salmonella, Shigella, Vibrio cholerae, Campylobacter, Staphylococcus, Rotavirus among others that are generally contained in feces, thus configuring a FECAL-ORAL type of transmission.
Among the factors that lead to the occurrence of gastrointestinal infections are the hygienic and sanitary deficiencies that characterize our markets and other places where raw or cooked food is sold, poor environmental sanitation in communities, deficiencies in water treatment (or in the process of its plumbing), risky hygienic-sanitary habits (not washing hands after major and/or minor needs), among others.
These are generally consequences (signs and symptoms) resulting from gastrointestinal infections: diarrhea, vomiting, fever and malaise, among others.
The treatment consists of replacing lost liquids and electrolytes (drinking drinking water and other recommended liquids, including consumption of juicy fruits such as papayas, apples, pears, among others that contain water in their composition).
To prevent this, it is necessary to promote health education, improve the hygienic-sanitary conditions of markets and communities in general as a way of promoting, preserving and prolonging PUBLIC HEALTH.
Gastritis and Gastric Health
Gastric Health is one of the most relevant concerns in human health, with gastrointestinal infections being among the main illnesses that affect humans.
Among gastric problems, we have GASTRITIS AND GASTRIC ULCERS as the main public health problems. Gastritis and gastric ulcers normally result from inflammation and corrosion of the walls of the stomach (gastric mucosa) and are generally associated (caused) by the bacterium Helicobacter pylor, which, according to the literature, this bacterium settles on these walls (of the stomach) and starts to release urease that ends up altering the normal pH of the stomach (acid), which leads to inflammation and corrosion of the mucous membranes and consequent gastritis or ulcers, respectively.
In addition to bacterial infections, gastritis and gastric ulcers are associated with several factors, with emphasis on prolonged fasting, chemical substances including drugs, alcohol, foods with strong seasonings including chilli, which ends up causing inflammation of the stomach walls and/or corrosion. of the same, resulting in the appearance of wounds and consequent gastritis or ulcers, respectively.
Among patients with gastritis and/or ulcers, one of the dilemmas is associated with the foods to consume in order to minimize the sensation of pain and discomfort. Travel Clinic Cardiff: Health Advice for International Travelers
Travel Clinic Cardiff offers comprehensive travel health services, including vaccinations, travel advice, and preventive care for international travelers. Our expert team ensures you are well-prepared and protected for your journey, providing personalized consultations tailored to your destination. Conveniently located in Cardiff, we help you travel with confidence and peace of mind. Visit us: www.nxhealthcare.co.uk
RESPIRATORY DISEASES by bhavya kelavadiya
The Children are very vulnerable to get affected with respiratory disease.
In our country, the respiratory Disease conditions are consider as major cause for mortality and Morbidity in Child.
PGx Analysis in VarSeq: A User’s Perspective
Since our release of the PGx capabilities in VarSeq, we’ve had a few months to gather some insights from various use cases. Some users approach PGx workflows by means of array genotyping or what seems to be a growing trend of adding the star allele calling to the existing NGS pipeline for whole genome data. Luckily, both approaches are supported with the VarSeq software platform. The genotyping method being used will also dictate what the scope of the tertiary analysis will be. For example, are your PGx reports a standalone pipeline or would your lab’s goal be to handle a dual-purpose workflow and report on PGx + Diagnostic findings.
The purpose of this webcast is to:
Discuss and demonstrate the approaches with array and NGS genotyping methods for star allele calling to prep for downstream analysis.
Following genotyping, explore alternative tertiary workflow concepts in VarSeq to handle PGx reporting.
Moreover, we will include insights users will need to consider when validating their PGx workflow for all possible star alleles and options you have for automating your PGx analysis for large number of samples. Please join us for a session dedicated to the application of star allele genotyping and subsequent PGx workflows in our VarSeq software.
How to choose the best dermatologists in Indore.
The skin is the largest organ and its health plays a vital role among the other sense organs. The skin concerns like acne breakout, psoriasis, or anything similar along the lines, finding a qualified and experienced dermatologist becomes paramount.
Debunking Nutrition Myths: Separating Fact from Fiction"
In a world overflowing with diet trends and conflicting nutrition advice, it’s easy to get lost in misinformation. This article cuts through the noise to debunk common nutrition myths that may be sabotaging your health goals. From the truth about carbohydrates and fats to the real effects of sugar and artificial sweeteners, we break down what science actually says. Equip yourself with knowledge to make informed decisions about your diet, and learn how to navigate the complexities of modern nutrition with confidence. Say goodbye to food confusion and hello to a healthier you!
Ageing, the Elderly, Gerontology and Public Health
Challenges associated with ageing from a public health perspective
Recently uploaded (20)
Nano-gold for Cancer Therapy chemistry investigatory project
Nano-gold for Cancer Therapy chemistry investigatory project
acne vulgaris -Mpharm (2nd semester) Cosmetics and cosmeceuticals
acne vulgaris -Mpharm (2nd semester) Cosmetics and cosmeceuticals
Helminthiasis or Worm infestation in Children for Nursing students
Helminthiasis or Worm infestation in Children for Nursing students
Call Girls In Mumbai +91-7426014248 High Profile Call Girl Mumbai
Call Girls In Mumbai +91-7426014248 High Profile Call Girl Mumbai
Demystifying Fallopian Tube Blockage- Grading the Differences and Implication...
Demystifying Fallopian Tube Blockage- Grading the Differences and Implication...
Medical Quiz ( Online Quiz for API Meet 2024 ).pdf
Medical Quiz ( Online Quiz for API Meet 2024 ).pdf
Osvaldo Bernardo Muchanga-GASTROINTESTINAL INFECTIONS AND GASTRITIS-2024.pdf
Osvaldo Bernardo Muchanga-GASTROINTESTINAL INFECTIONS AND GASTRITIS-2024.pdf
Travel Clinic Cardiff: Health Advice for International Travelers
Travel Clinic Cardiff: Health Advice for International Travelers
Debunking Nutrition Myths: Separating Fact from Fiction"
Debunking Nutrition Myths: Separating Fact from Fiction"
Ageing, the Elderly, Gerontology and Public Health
Ageing, the Elderly, Gerontology and Public Health
Epidermoid cyst
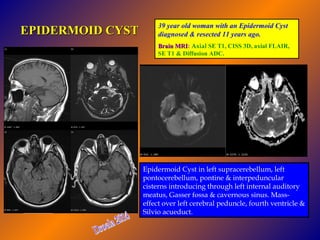
- 1. EPIDERMOID CYST 39 year old woman with an Epidermoid Cyst diagnosed & resected 11 years ago. Brain MRI: Axial SE T1, CISS 3D, axial FLAIR, MRI SE T1 & Diffusion ADC. Epidermoid Cyst in left supracerebellum, left pontocerebellum, pontine & interpeduncular cisterns introducing through left internal auditory meatus, Gasser fossa & cavernous sinus. Masseffect over left cerebral peduncle, fourth ventricle & Silvio acueduct.