Downloaded 177 times

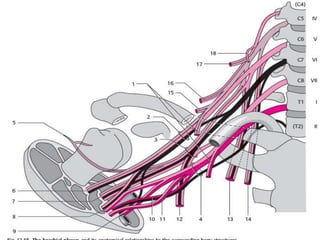
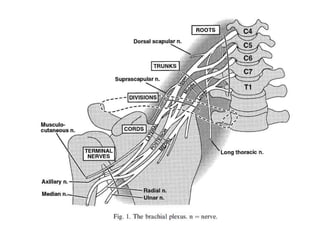
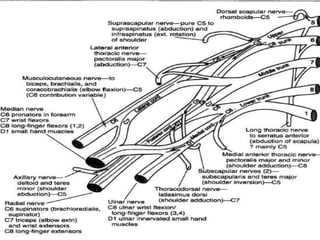
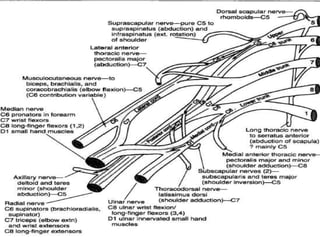
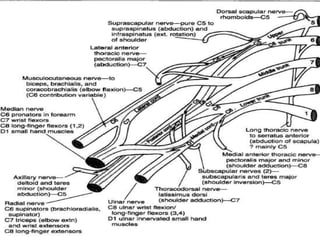
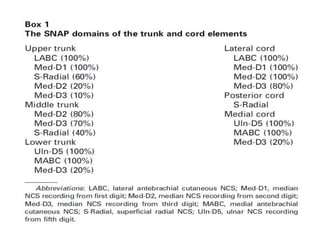
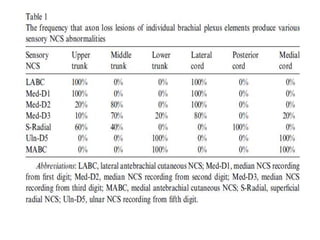
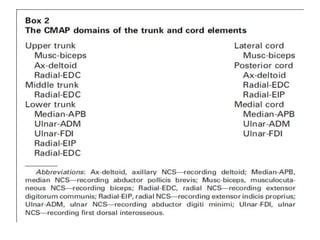
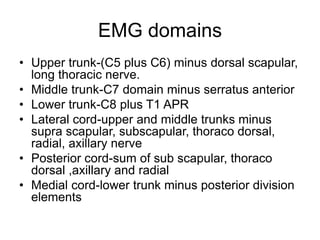
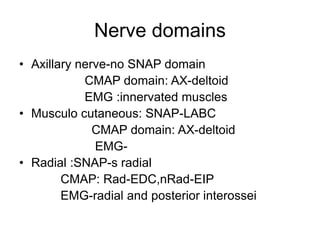
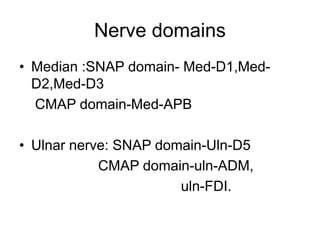
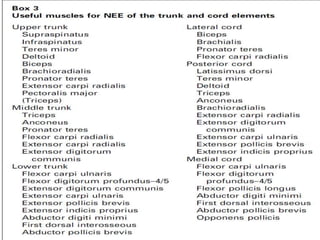
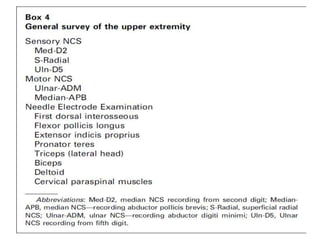

This document discusses the electrophysiological evaluation of the brachial plexus using nerve conduction studies and electromyography. It describes the anatomy of the brachial plexus including its roots, trunks, divisions, cords, and terminal nerves. It explains how to assess each element of the brachial plexus using sensory nerve action potentials, compound muscle action potentials, and electromyography findings. It also discusses the patterns seen with different types of brachial plexus lesions and provides guidance on timing of electrodiagnostic testing and prognostication.























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









