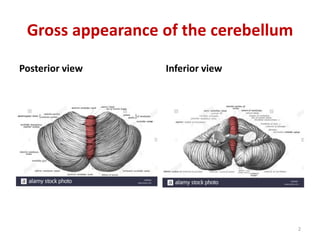
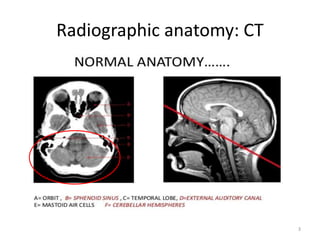
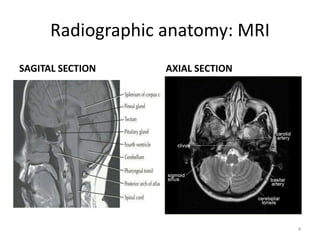
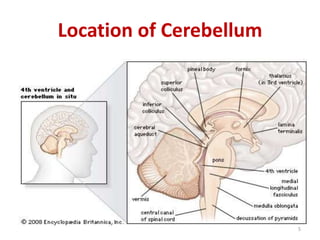
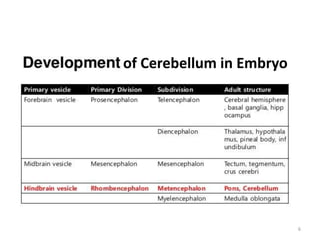
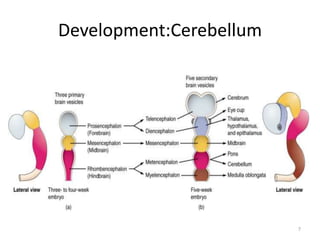
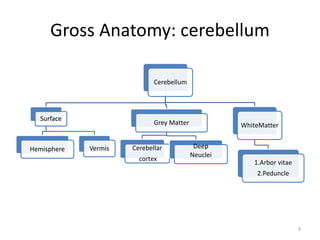
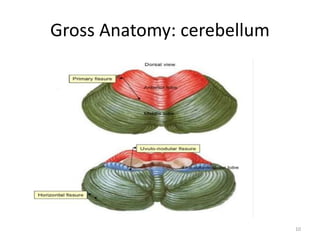
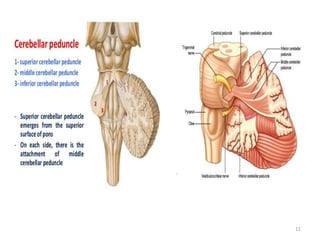
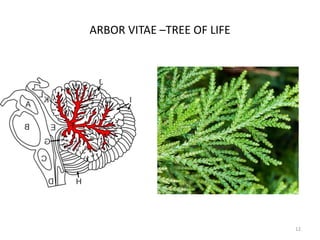
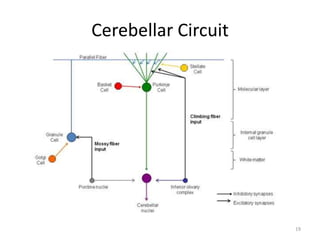
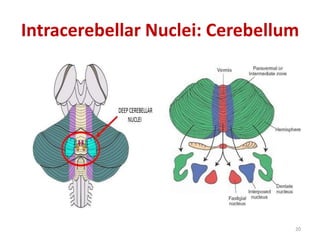
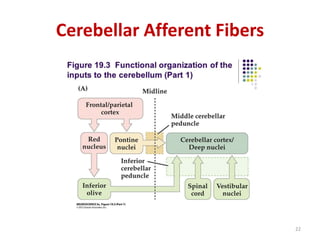
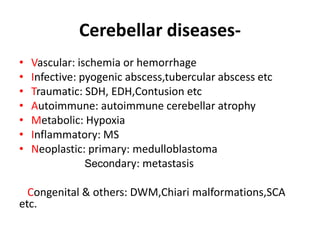
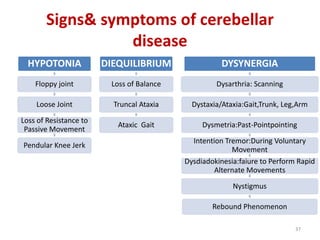
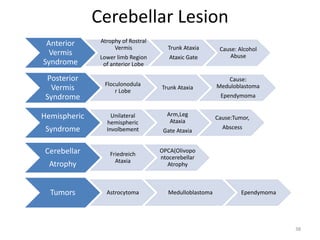
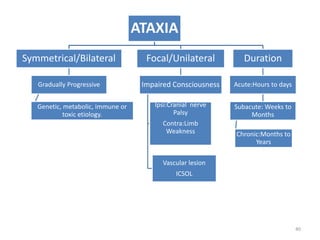
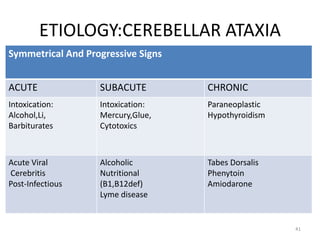
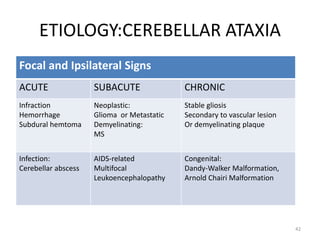
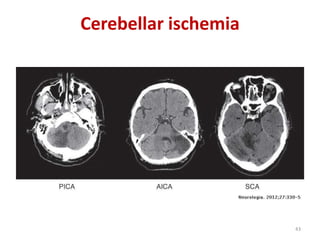
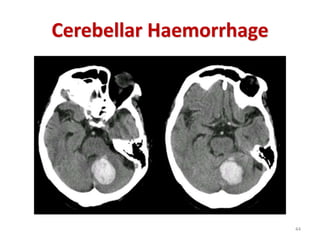
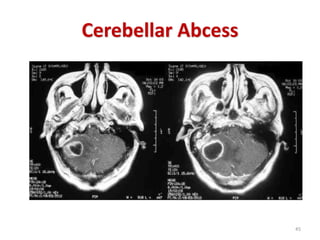
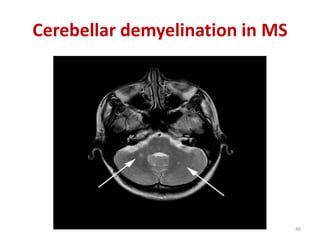
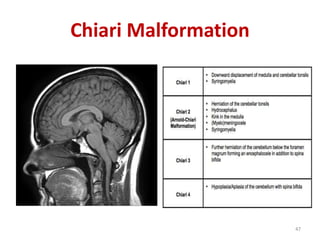
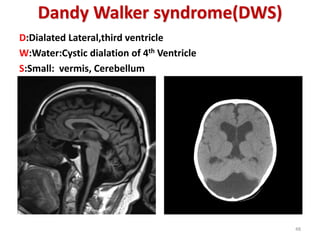
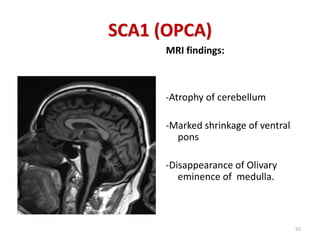
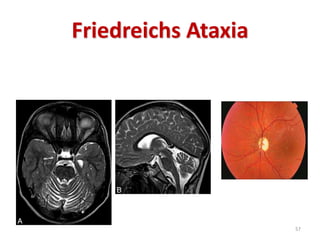
This document provides an overview of the cerebellum. It discusses the gross anatomy, radiographic appearance, development, functional divisions, blood supply, and common pathologies of the cerebellum. Key points covered include the connections between the cerebellum and brainstem, the cortical layers and circuitry, the phylogenetic and functional roles of different cerebellar regions, and common causes of cerebellar ataxia including vascular, infectious, autoimmune, metabolic, neoplastic and inherited etiologies. Diagrams are provided to illustrate cerebellar anatomy and examples of various cerebellar lesions.