Downloaded 86 times


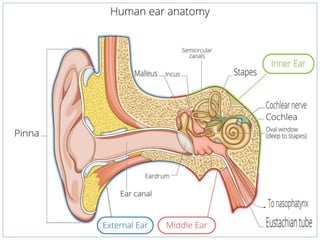
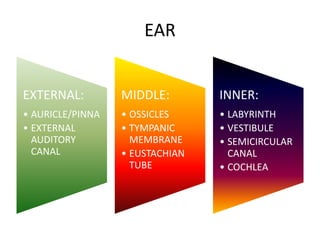









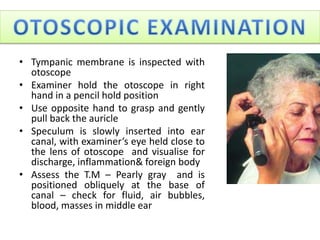



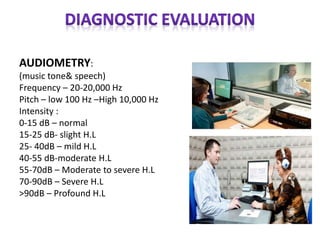



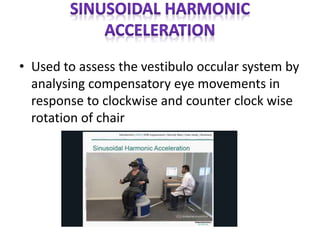


The document summarizes the anatomy and examination of the ear. It describes the external, middle, and inner ear structures. Examination techniques are outlined including otoscopy, tuning fork tests, whisper test, and audiometry. Additional tests mentioned are tympanometry, BERA, VNG, and rotary chair testing to evaluate hearing and balance functions of the ear.






















































































