Downloaded 131 times
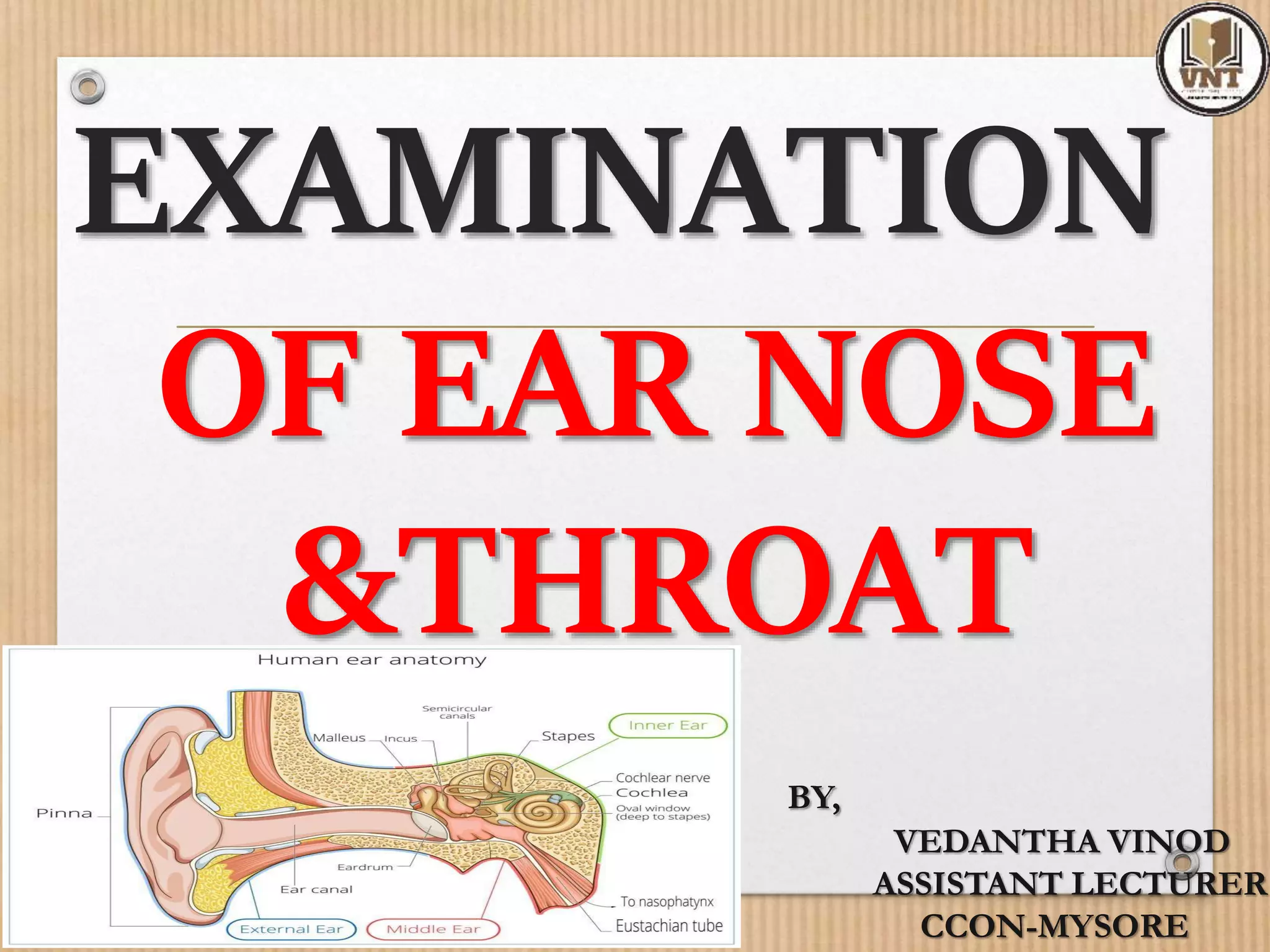
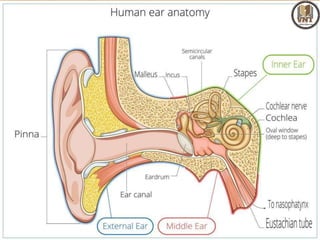
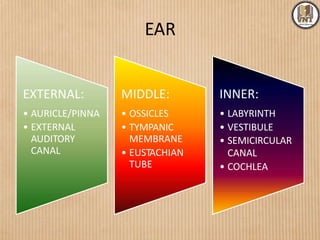
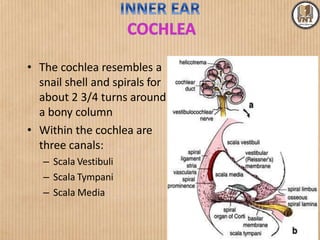


This document details the examination procedures for the ear, nose, and throat (ENT), including anatomy, history-taking, and inspection techniques. It covers components of the outer, middle, and inner ear, the importance of earwax, various otoscopic examination methods, and assessment techniques for nasal and throat conditions. The document emphasizes the significance of symptoms and medical history in diagnosing ENT-related issues.







































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














