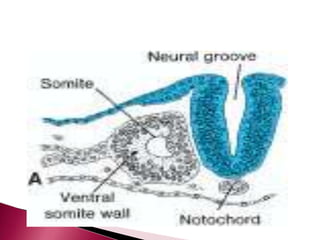
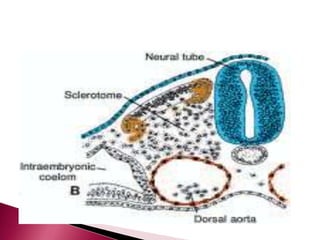
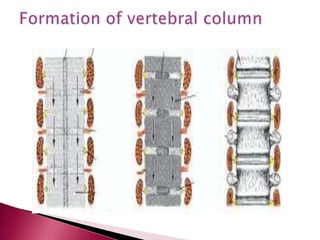
The document discusses the development of the vertebral column and ribs from sclerotome portions of somites. Sclerotome cells migrate and resegment to form vertebrae consisting of vertebral bodies and processes. Intervertebral discs form from mesenchymal cells between vertebrae. Defects like scoliosis can occur if vertebrae fuse asymmetrically. Ribs derive from sclerotome and cartilage, while the sternum develops from lateral plate mesoderm fusing in the midline, and may exhibit defects like cleft sternum.