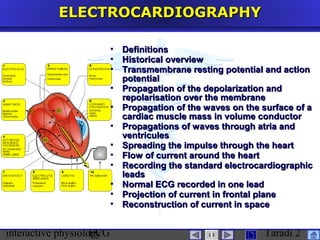
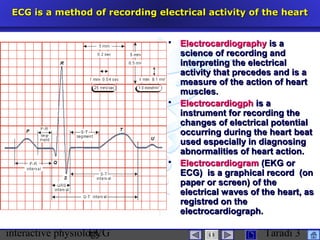
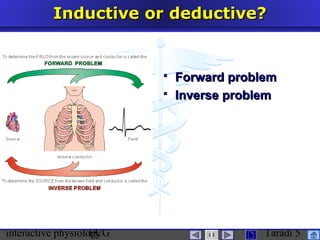
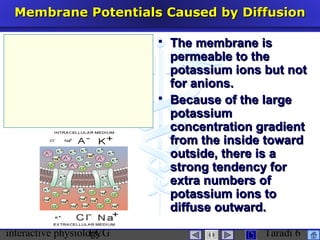
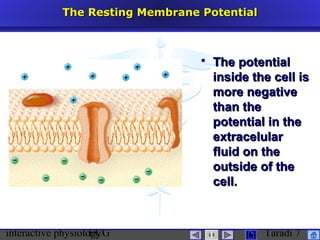
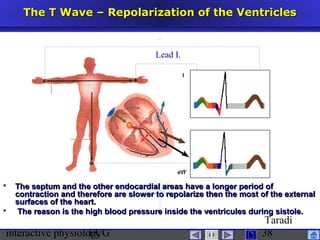
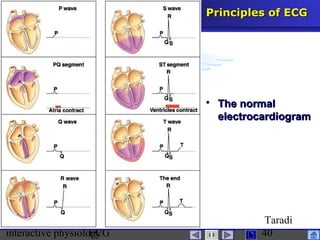
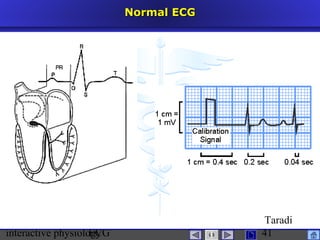
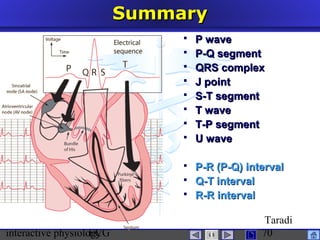
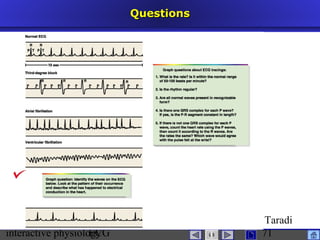
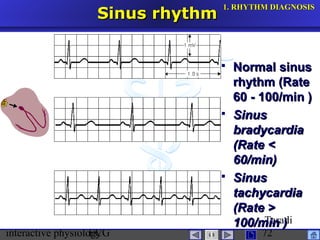
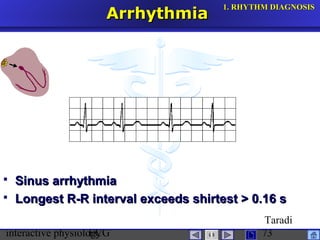
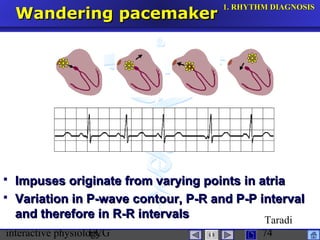
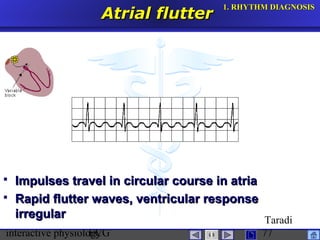

The document discusses electrocardiography (ECG), which is a method for recording the electrical activity of the heart. It provides definitions of ECG and electrocardiogram. It then covers the historical development of ECG from early experiments in the 1800s to the invention of the electrocardiograph by Willem Einthoven in the early 1900s. The document goes on to discuss membrane potentials, action potentials, and how the propagation of electrical signals through the heart is recorded via ECG leads to analyze the heart's function.











































































































