Download to read offline
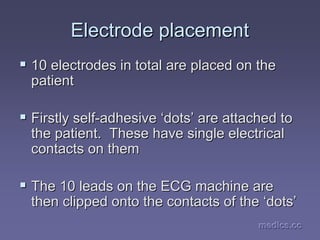
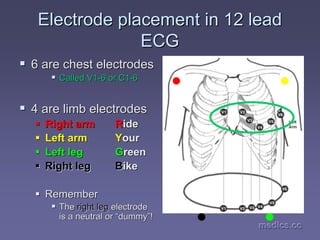
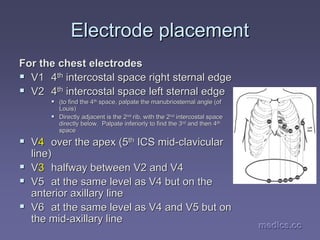
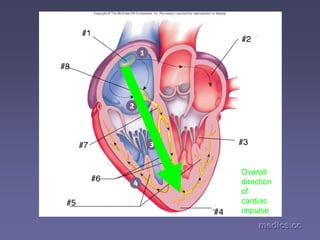
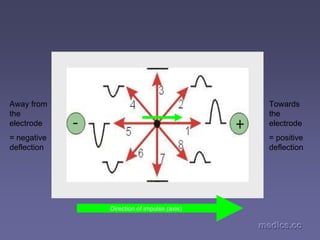
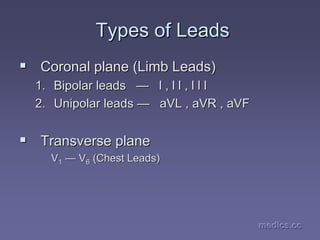
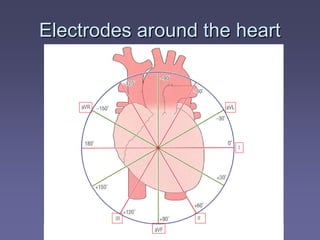
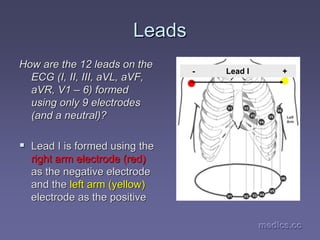
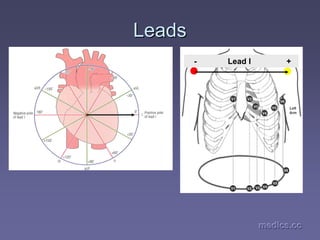
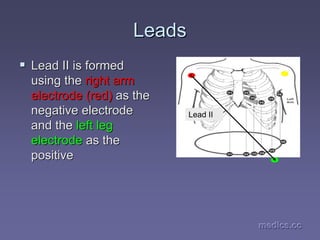
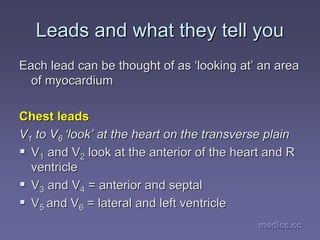
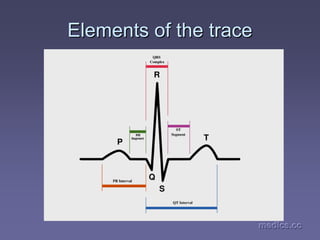
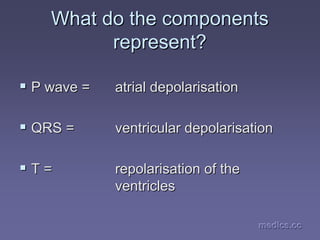



This document provides an overview of performing and interpreting electrocardiograms (ECGs). It outlines the objectives of understanding ECGs, including defining an ECG, performing one, and interpreting various cardiac pathologies. The document explains that an ECG is a tracing of the heart's electrical activity and describes the process for recording one, including electrode placement and the cardiac conduction system. It also provides a high-level overview of the typical waves, segments and intervals seen on an ECG tracing and how the different leads view the heart.










































































