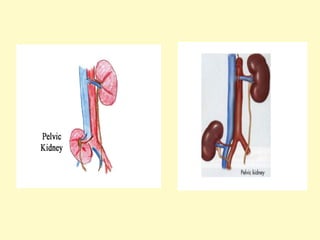
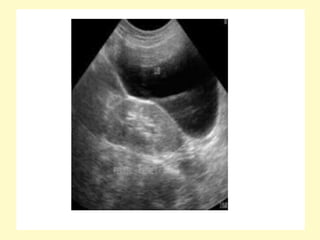
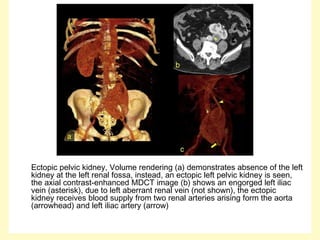
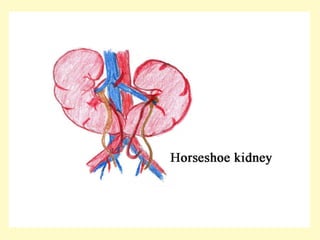
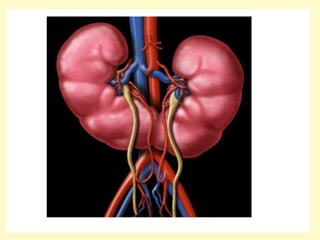
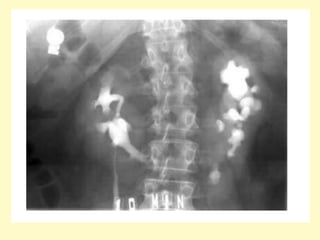
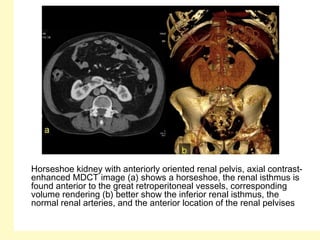
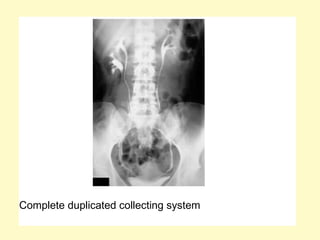
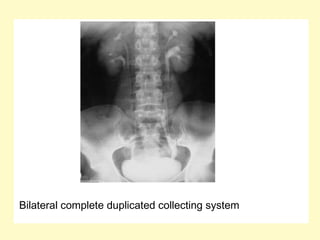
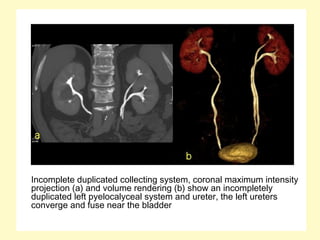
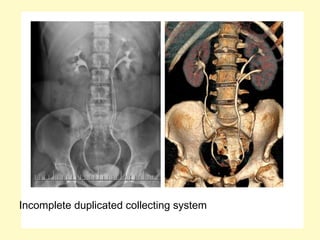
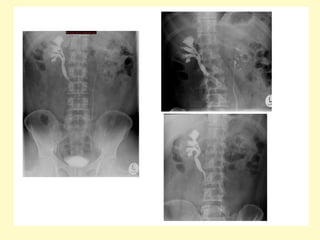
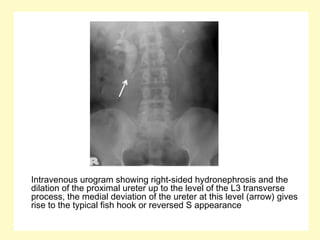
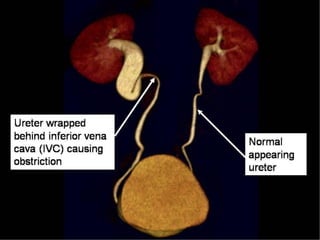
This document discusses various congenital anomalies of the genitourinary system, including anomalies related to position, form, number, vascular development, and bladder development of the kidneys and urinary tract. Specific anomalies covered include horseshoe kidney, ectopic kidney, renal agenesis, duplex collecting systems, retrocaval ureter, bladder duplication, exstrophy, and prune belly syndrome. Each anomaly is defined and relevant radiographic features are provided to aid in diagnosis.