1. Congenital anomalies of the kidney and urinary tract are abnormalities that develop before birth and can affect the structure and function of the kidneys and urinary system.
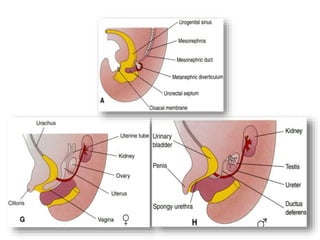
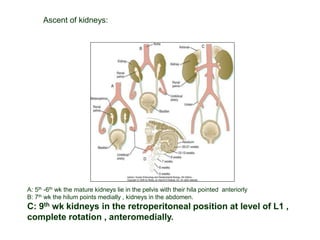
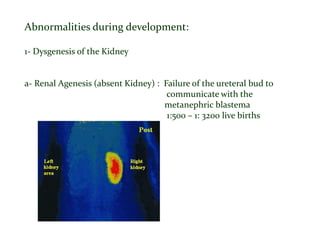
2. Some of the main anomalies discussed include renal agenesis (absent kidney), hypoplasia (small kidney), dysplasia (abnormal structure of kidney), and abnormalities in kidney position. Other anomalies affect the collecting system like duplex kidneys, hydronephrosis, and posterior urethral valves.
3. These anomalies can have various clinical presentations ranging from asymptomatic to end stage renal disease. They often require long term follow up and management to monitor renal and bladder function and address any complications. Bilateral involvement or