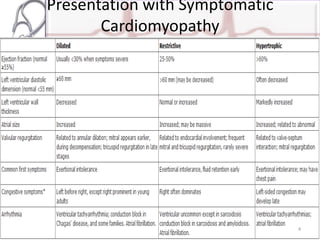
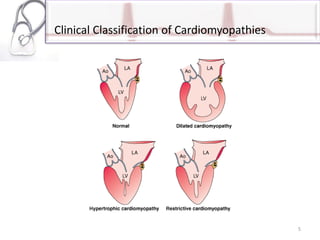
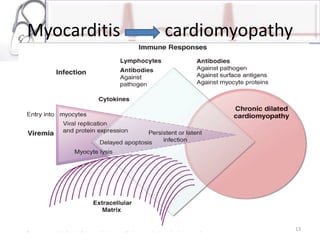
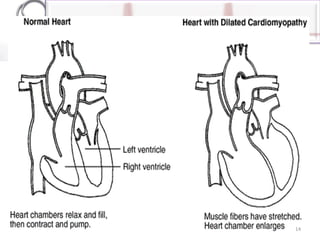
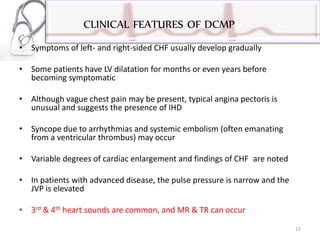
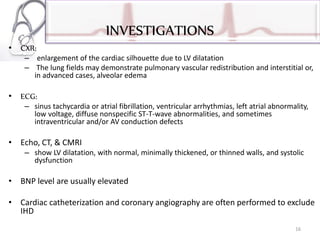
The document provides an overview of cardiomyopathies including definitions, classifications, presentations, evaluations, and treatments. It discusses the main types - dilated cardiomyopathy, hypertrophic cardiomyopathy, and restrictive cardiomyopathy. For dilated cardiomyopathy, it describes the etiologies, clinical features, investigations, and treatments. It notes dilated cardiomyopathy is the most common cardiomyopathic phenotype and often a final common pathway of cardiac injuries. For hypertrophic cardiomyopathy, it discusses the pathophysiology, clinical manifestations, investigations, and treatments including the use of beta-blockers and surgical procedures. For restrictive cardiomyopathy, it lists possible causes and notes the hallmark is abnormal diastolic function with excessive ventricular wall rig