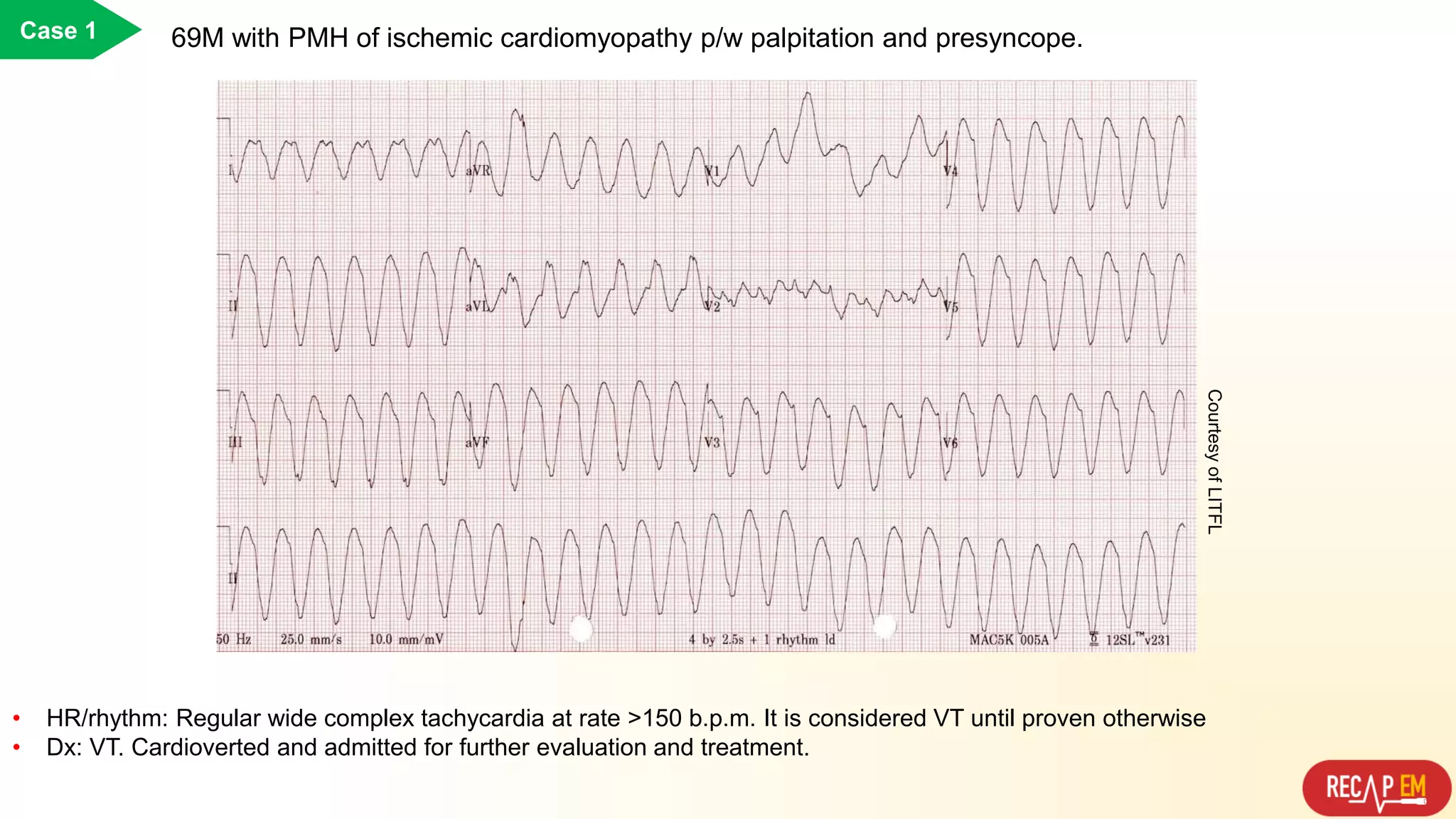
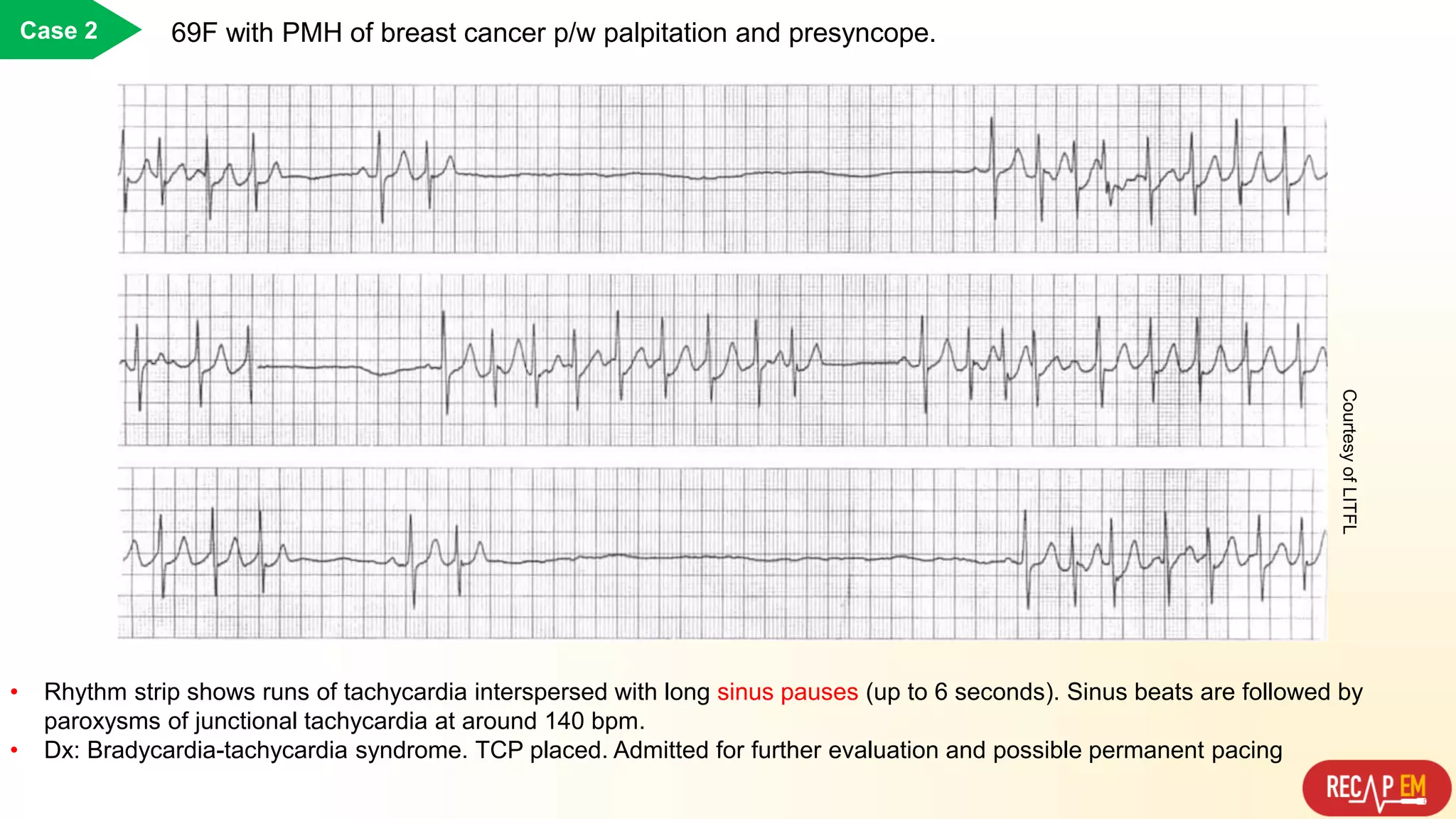
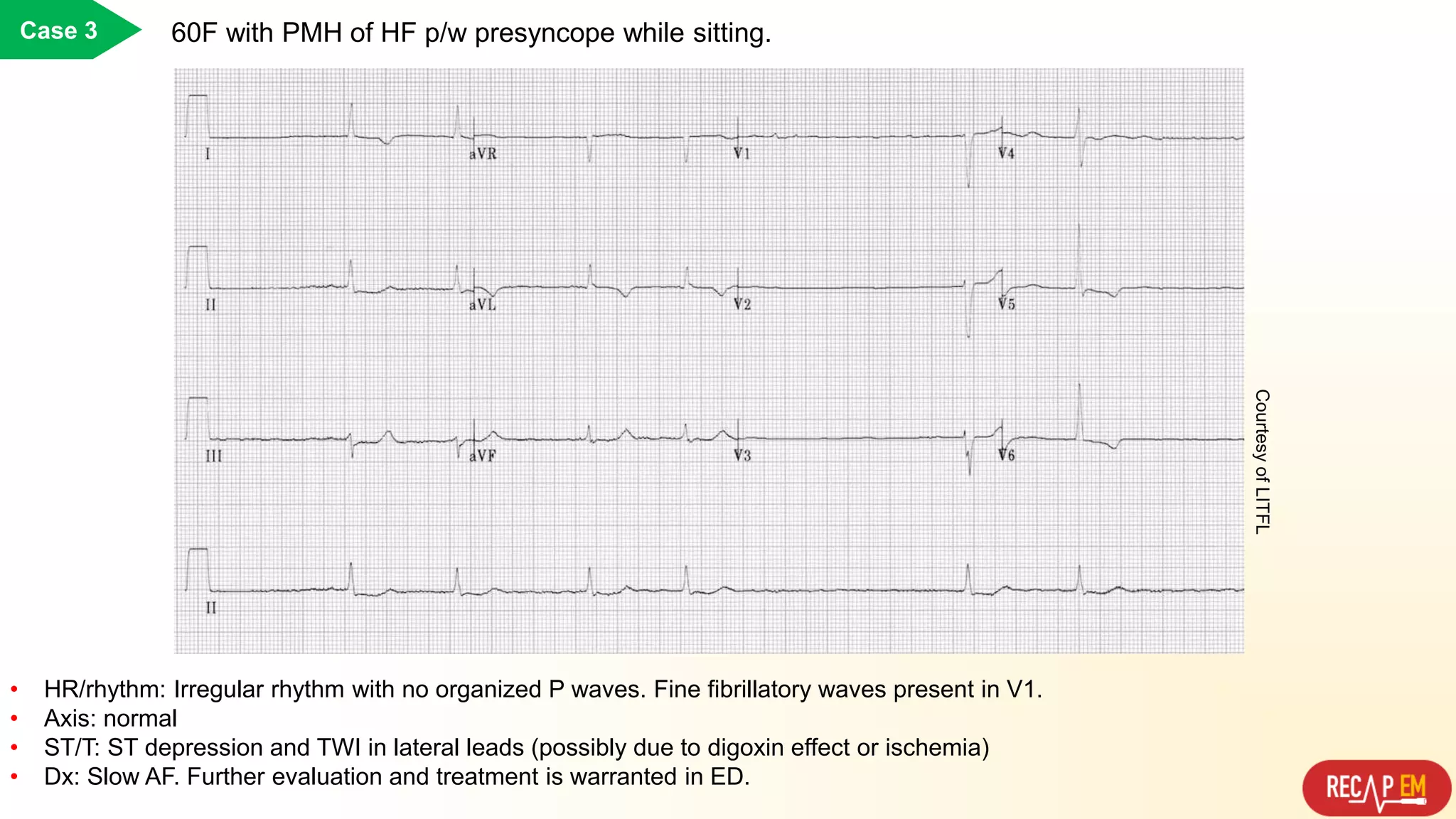
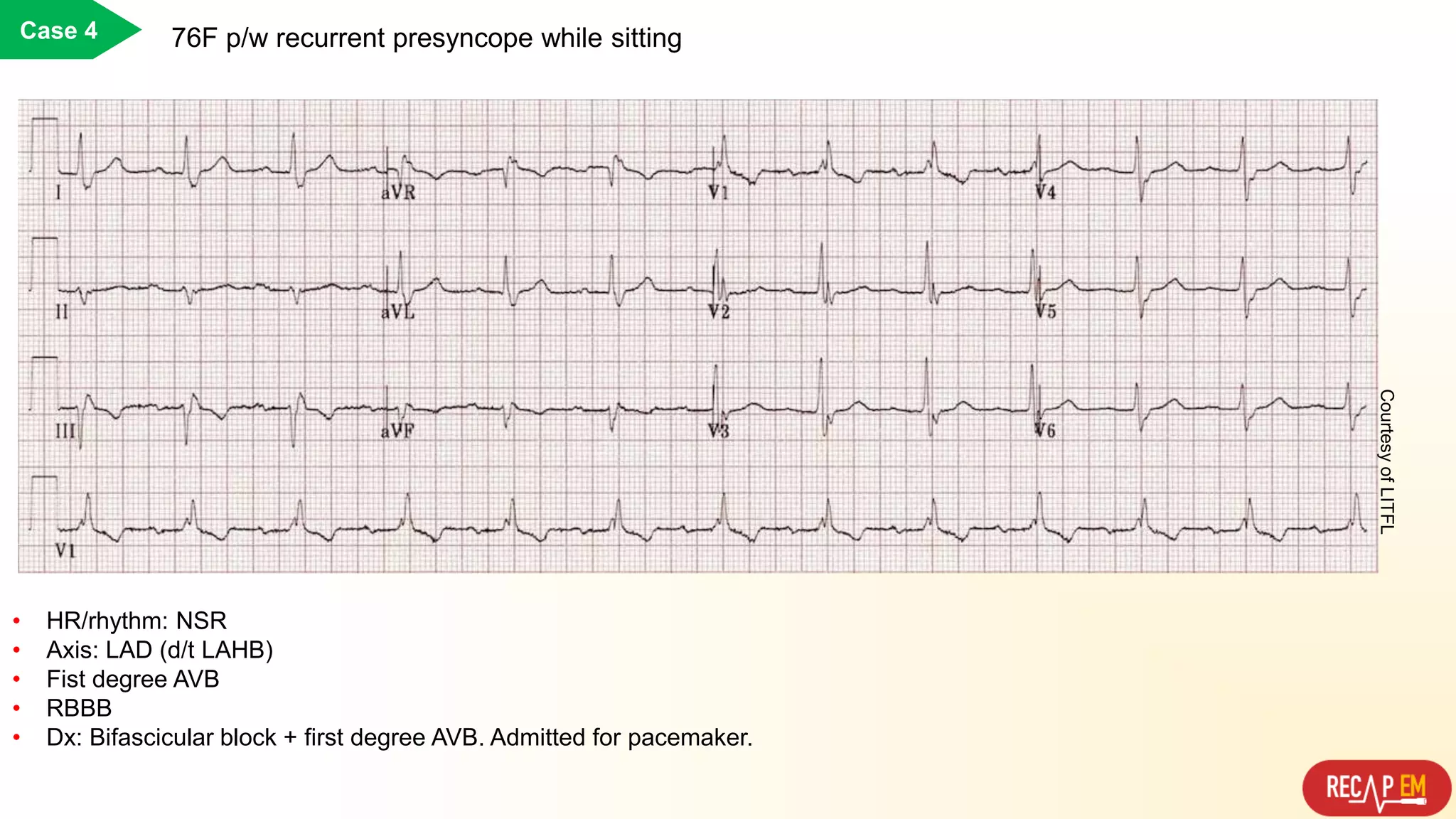
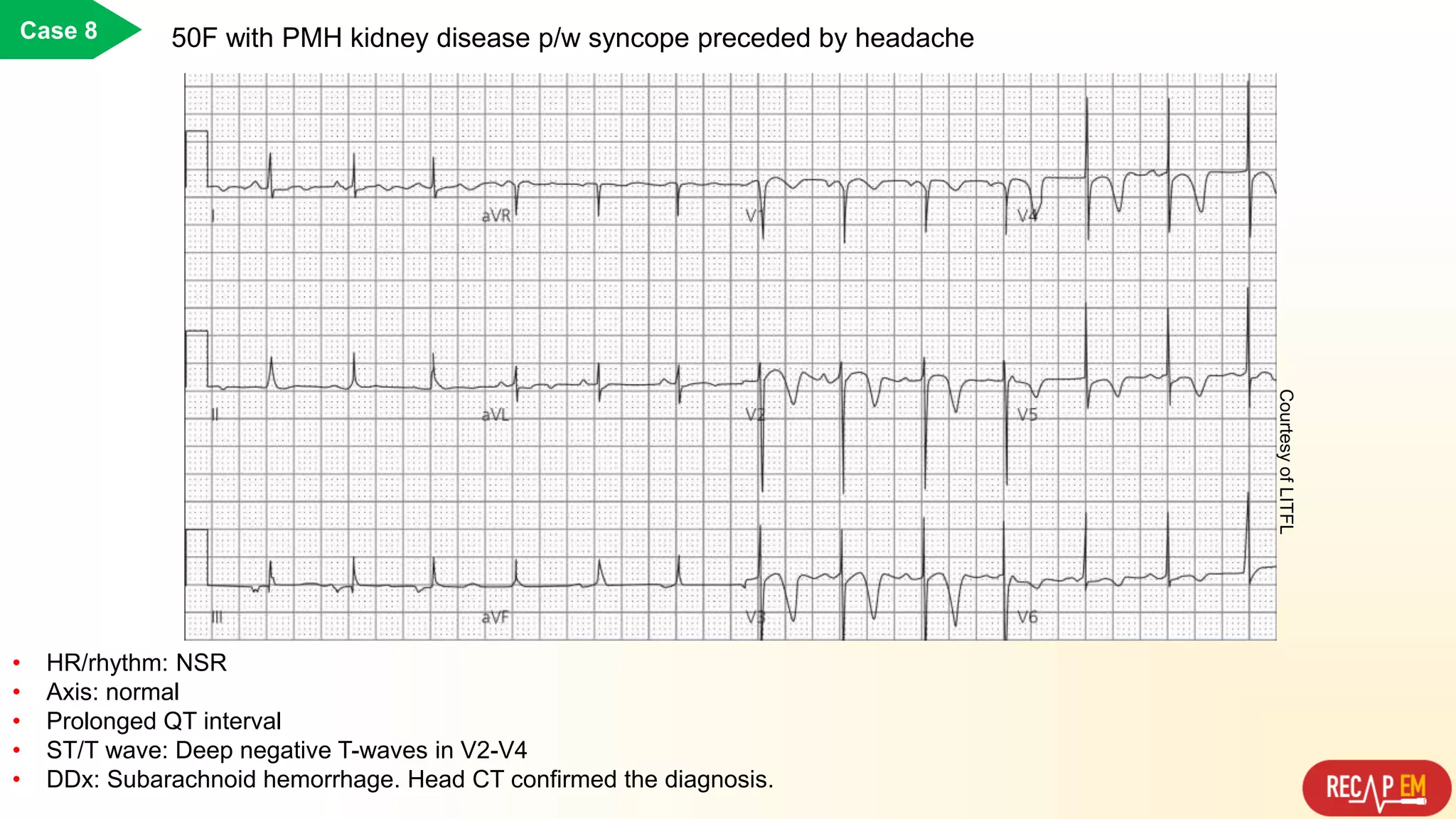
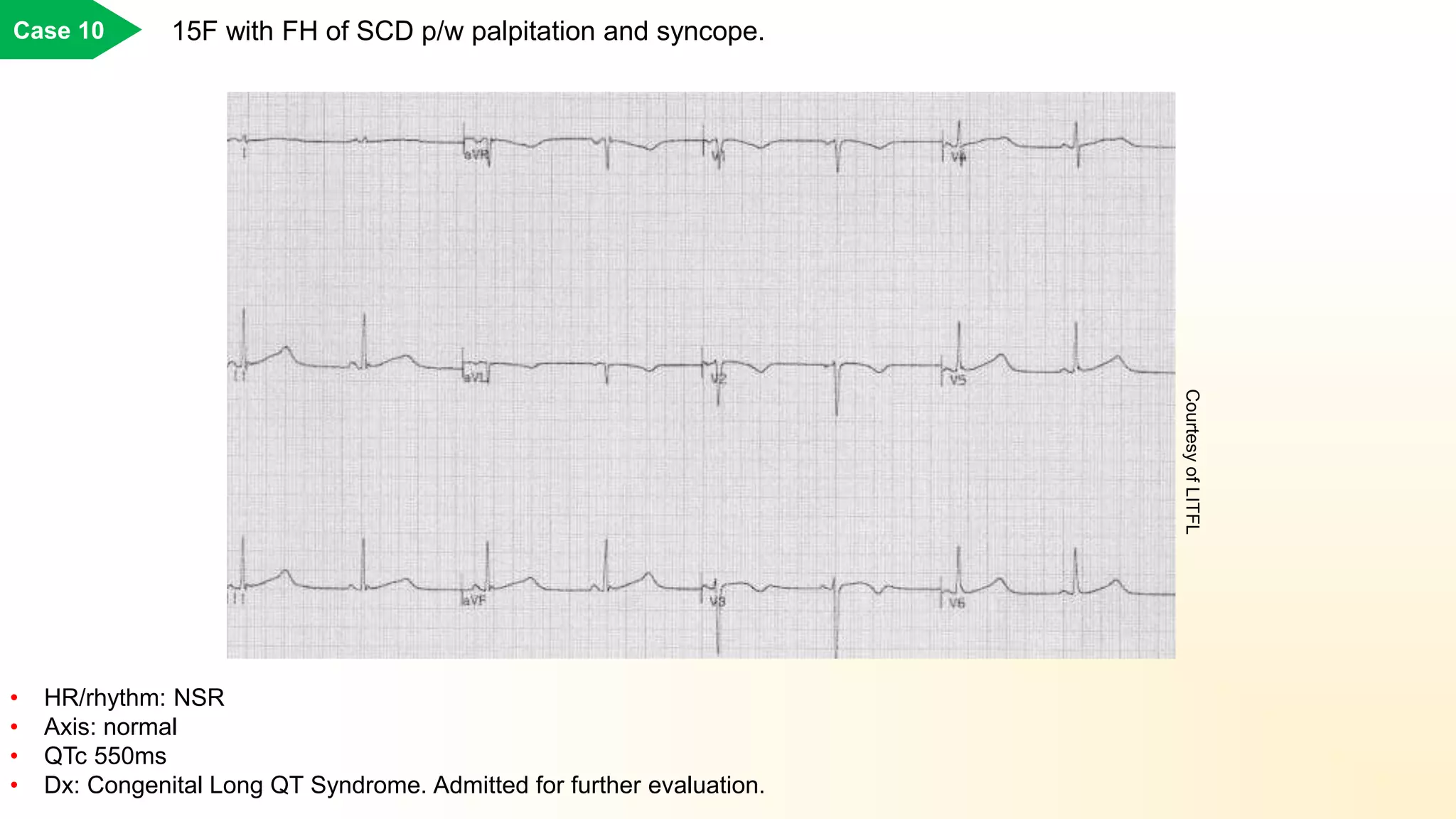
This document discusses key things to assess on an ECG for a patient presenting with syncope. It outlines 10 case examples assessing rate and rhythm, axis, intervals, voltages, and ST/T wave changes. The cases demonstrate various arrhythmias, conduction abnormalities, channelopathies, and structural heart diseases that can cause syncope including ventricular tachycardia, bradycardia-tachycardia syndrome, atrial fibrillation, bifascicular block, hypertrophic cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy, Brugada syndrome, subarachnoid hemorrhage, Wolff-Parkinson-White syndrome, and long QT syndrome.