Downloaded 88 times


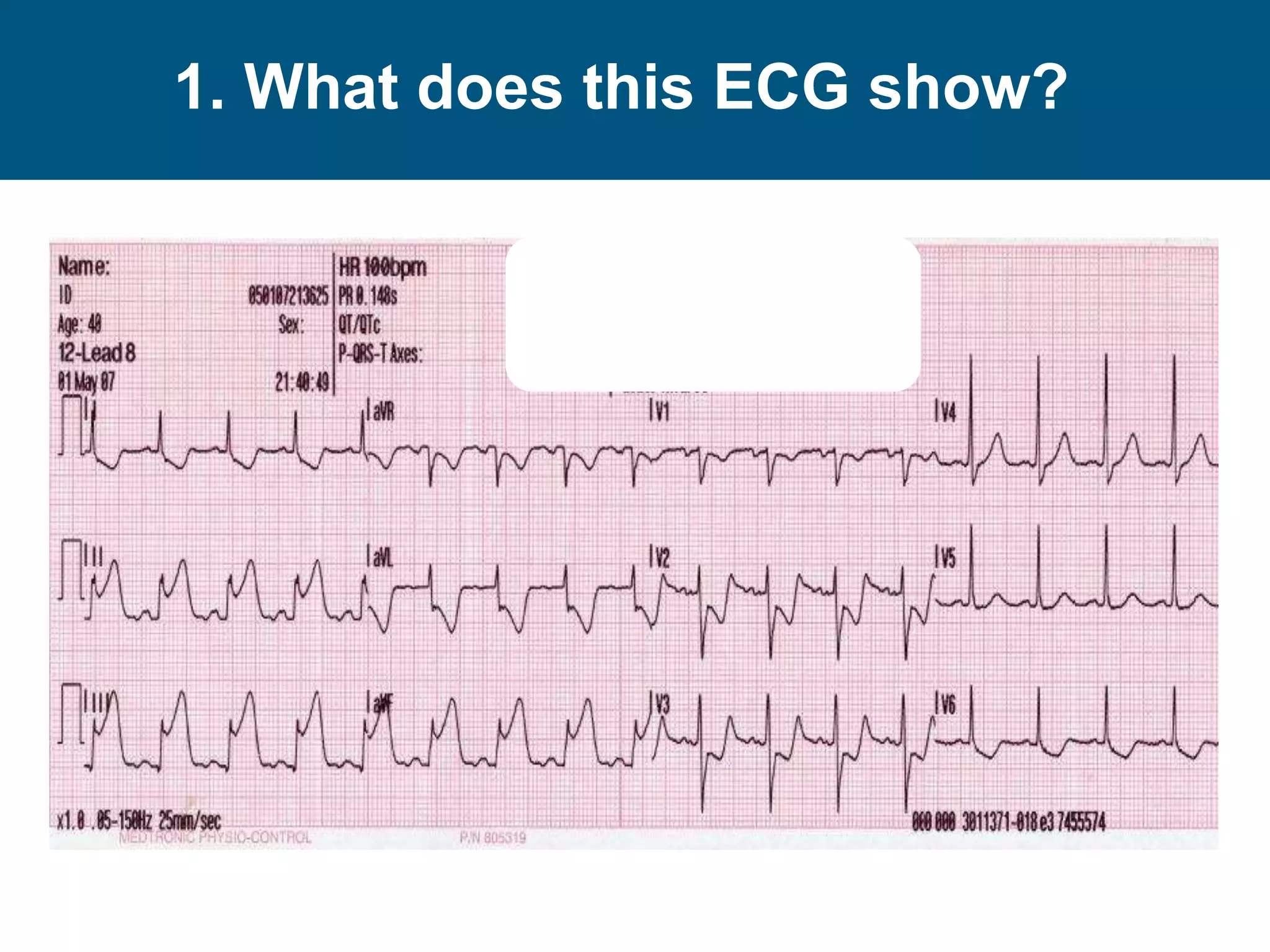
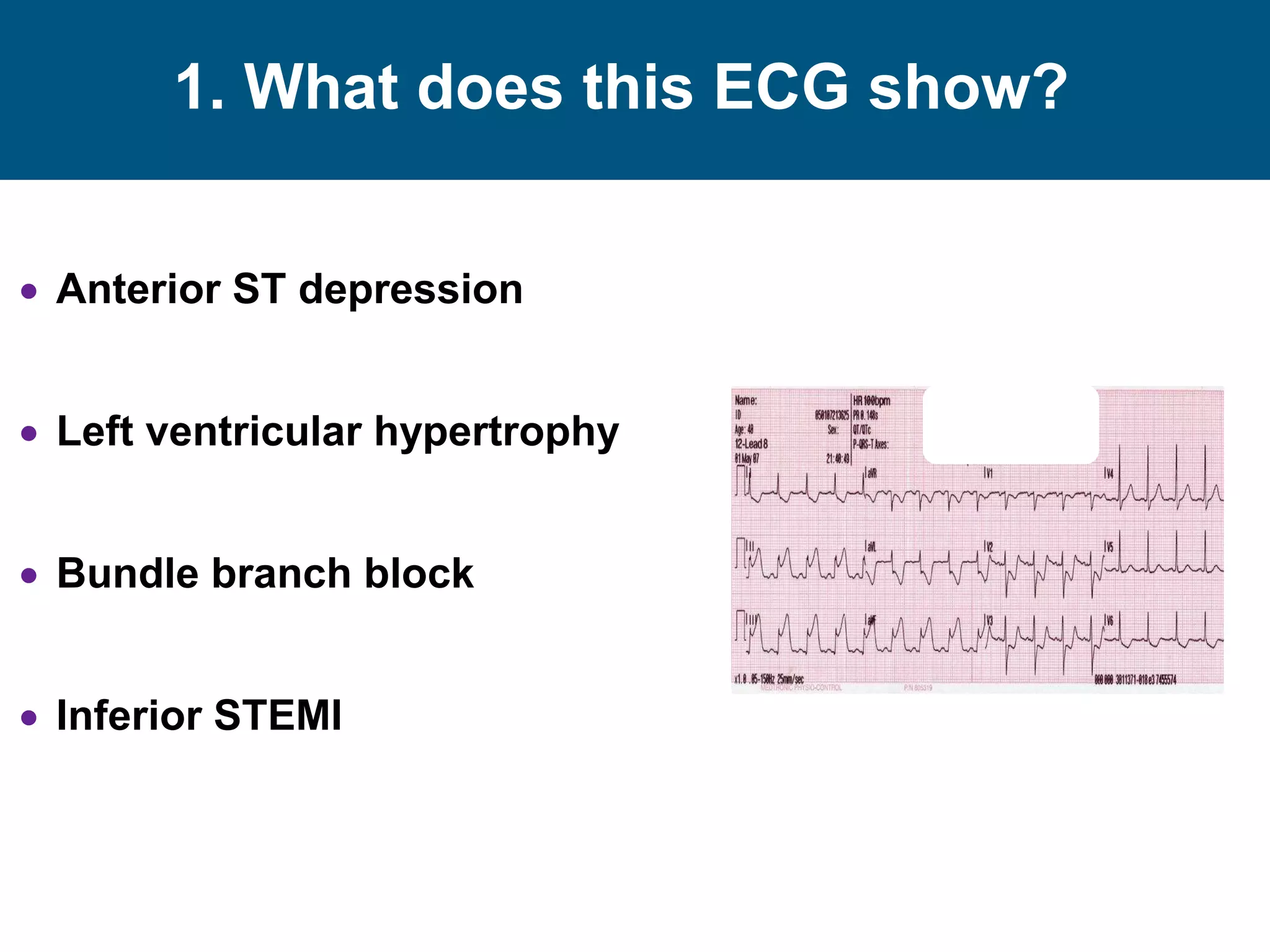

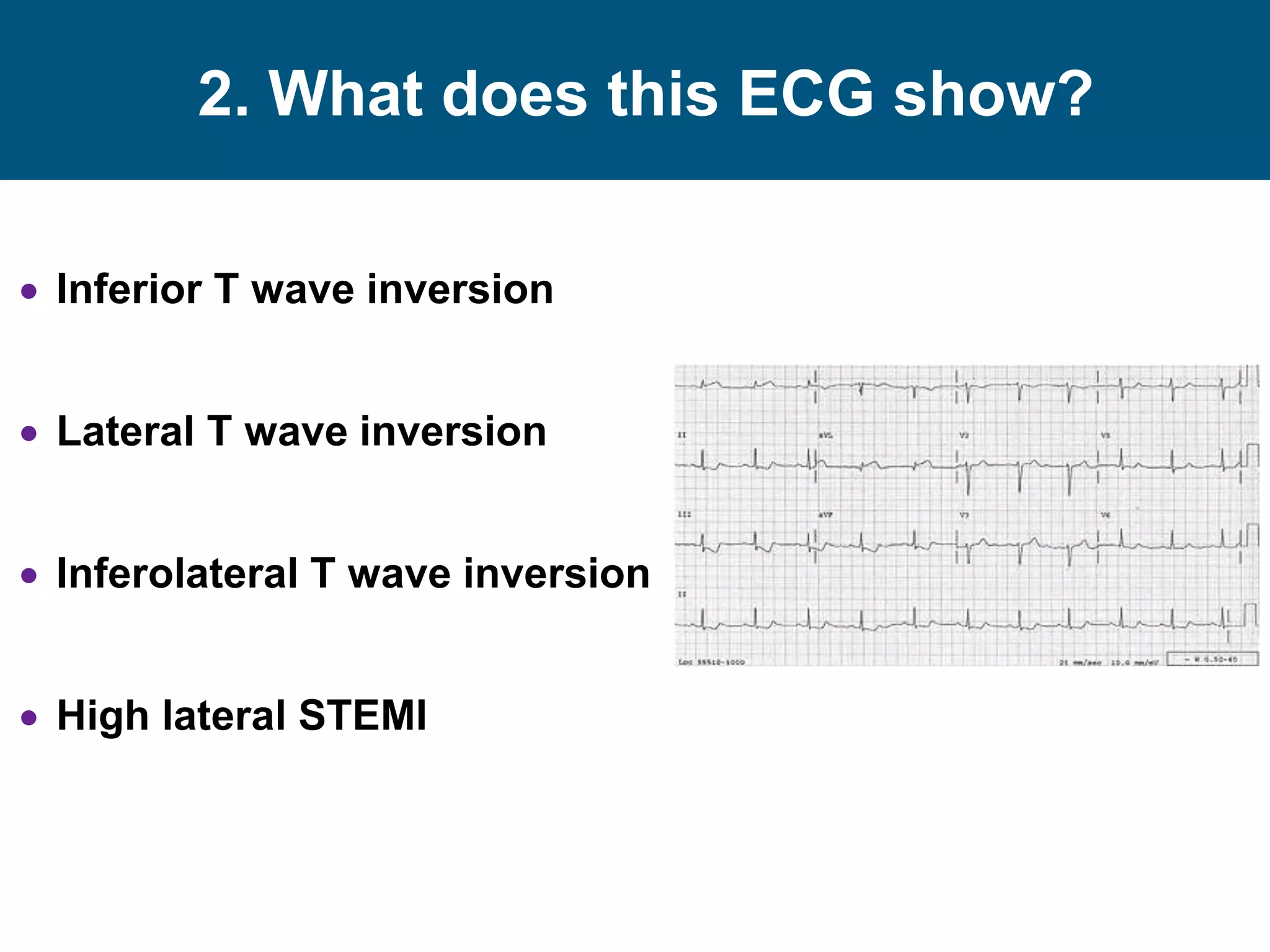


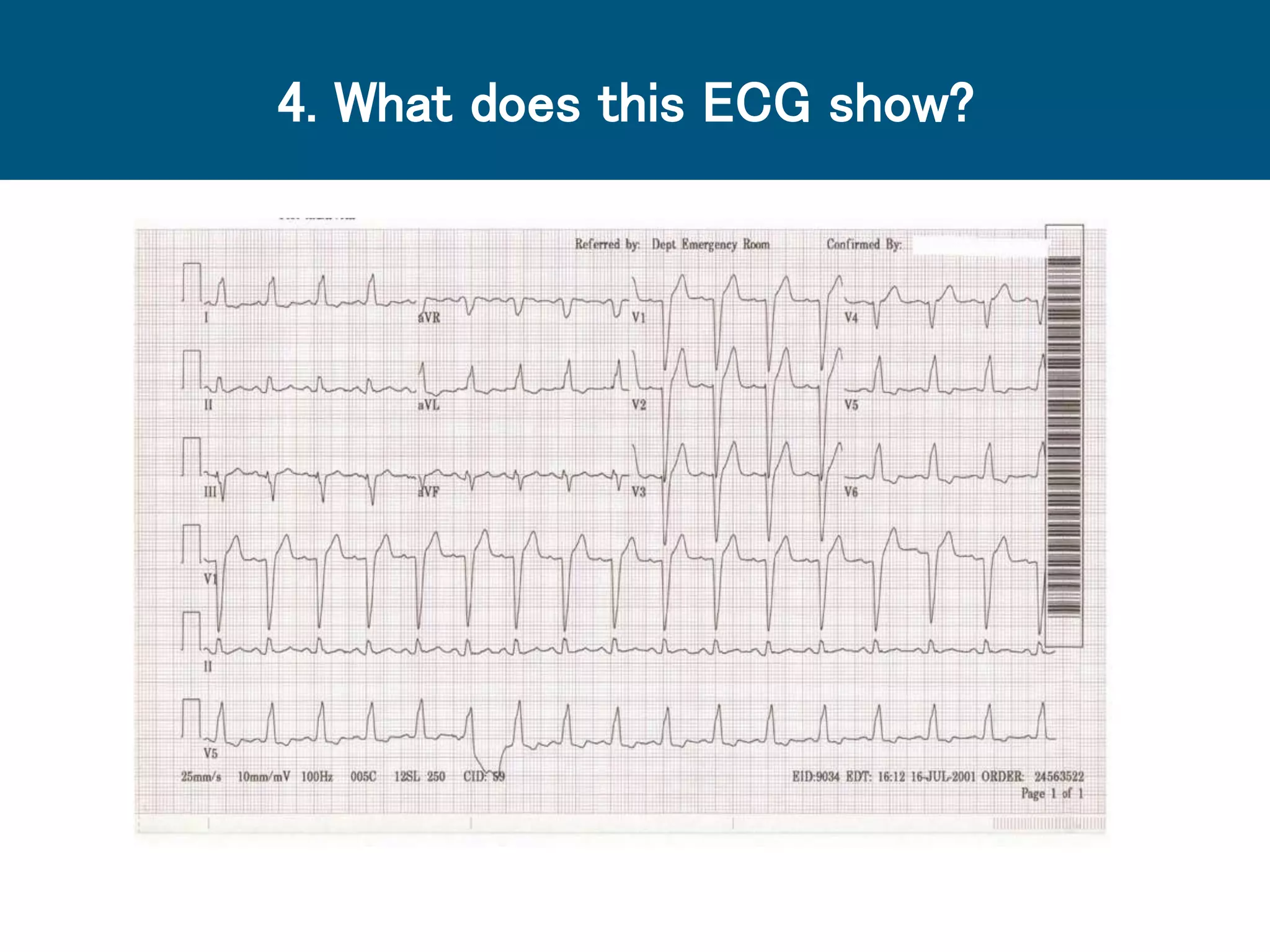
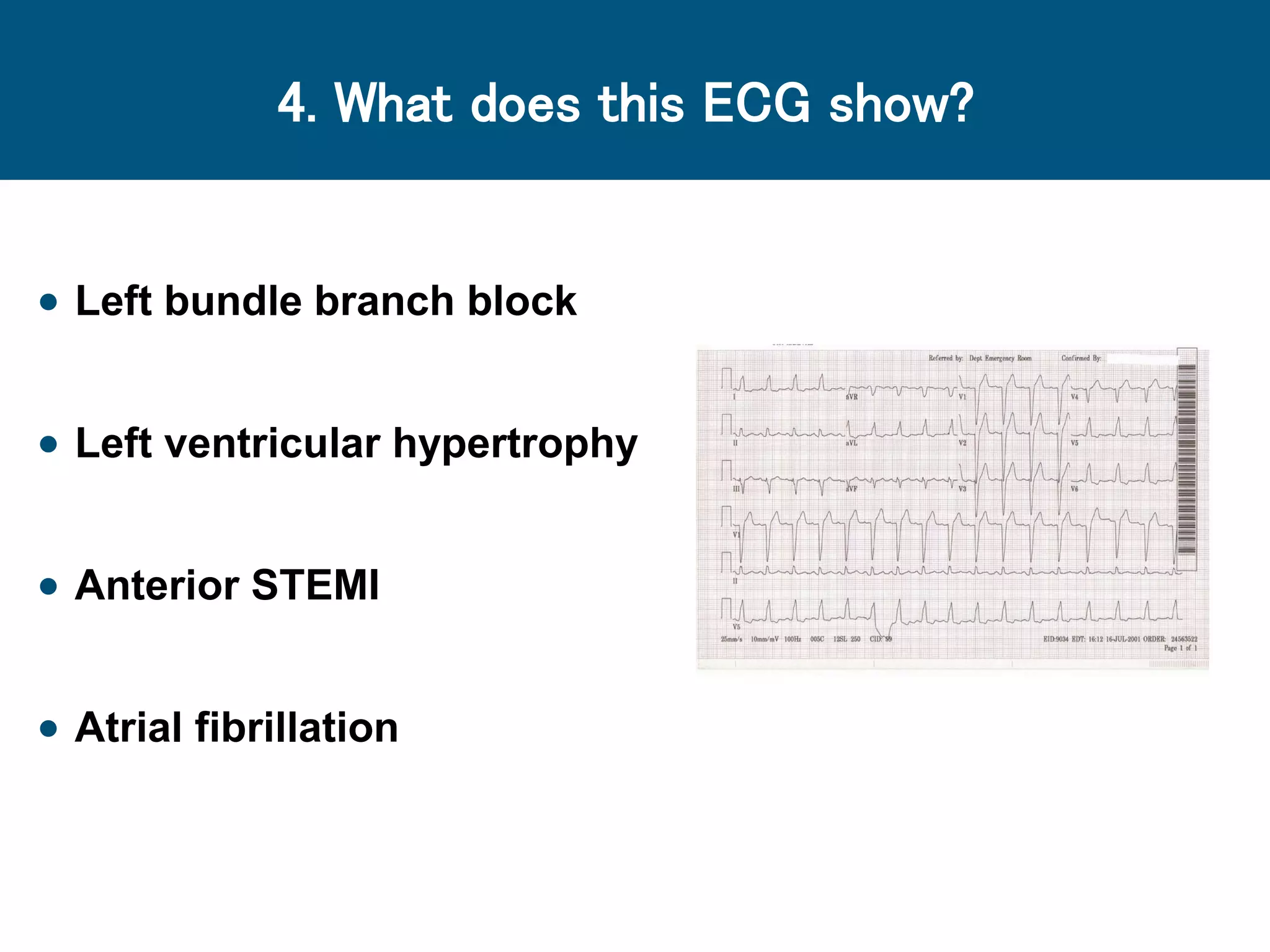







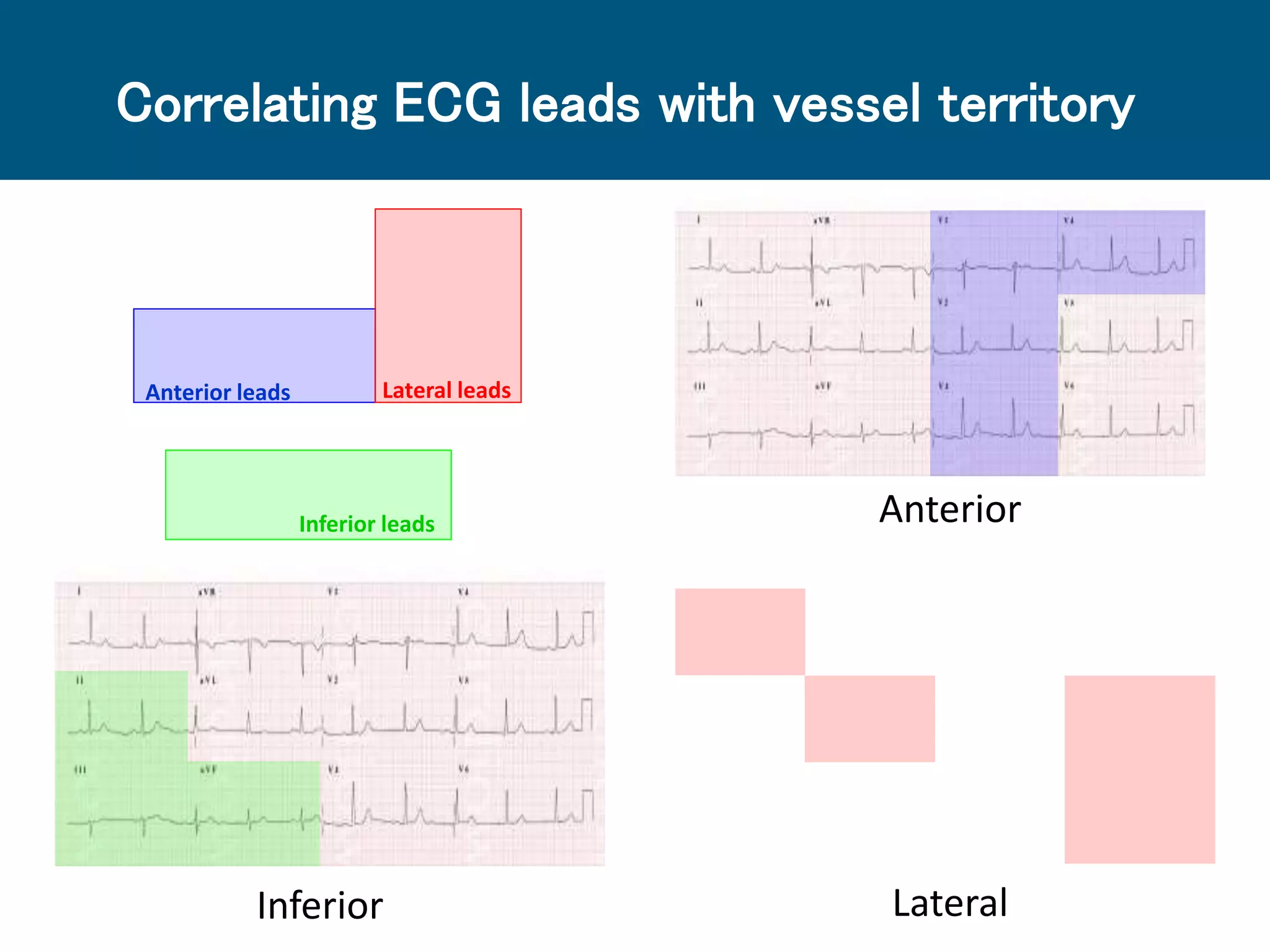
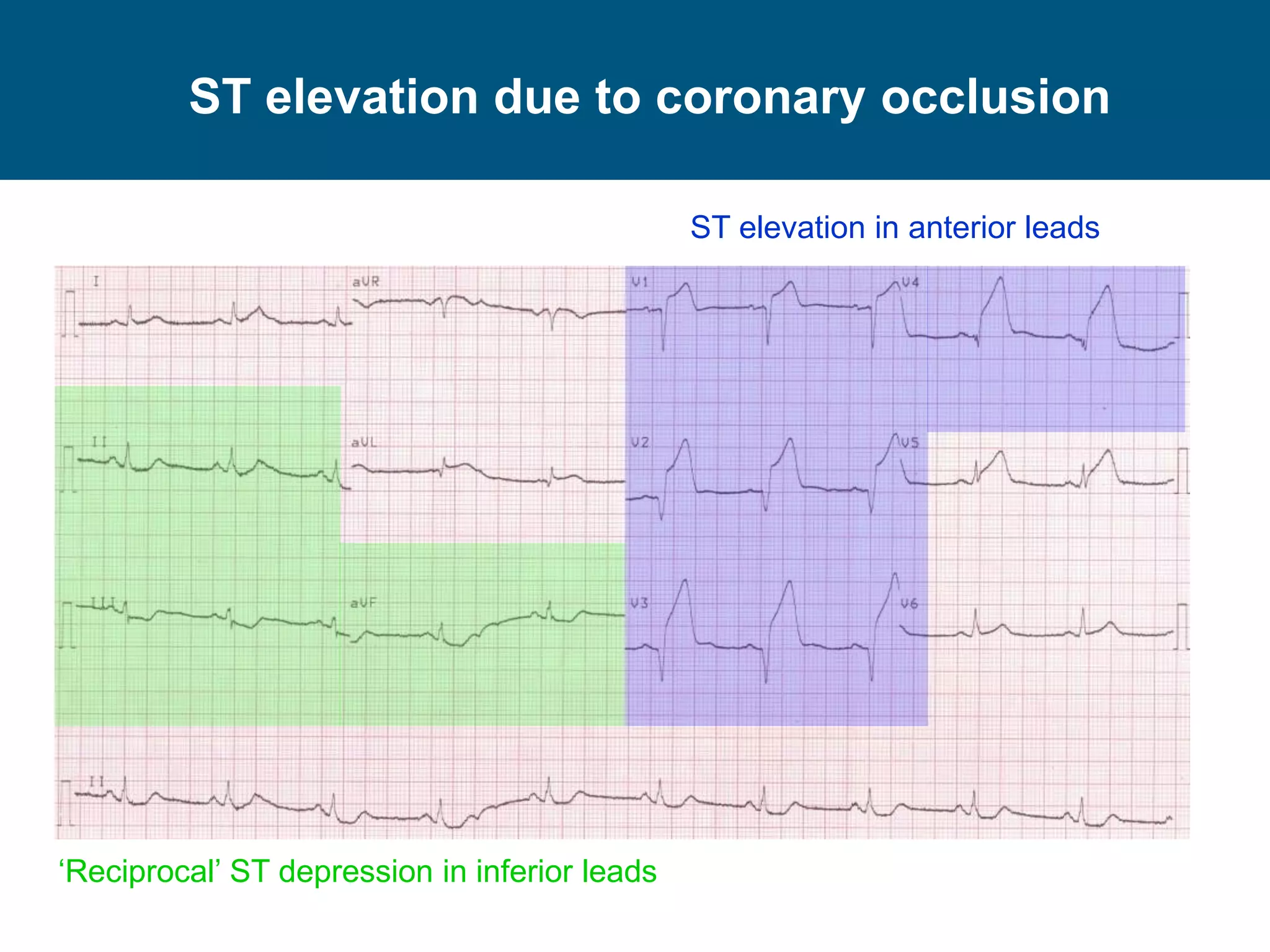
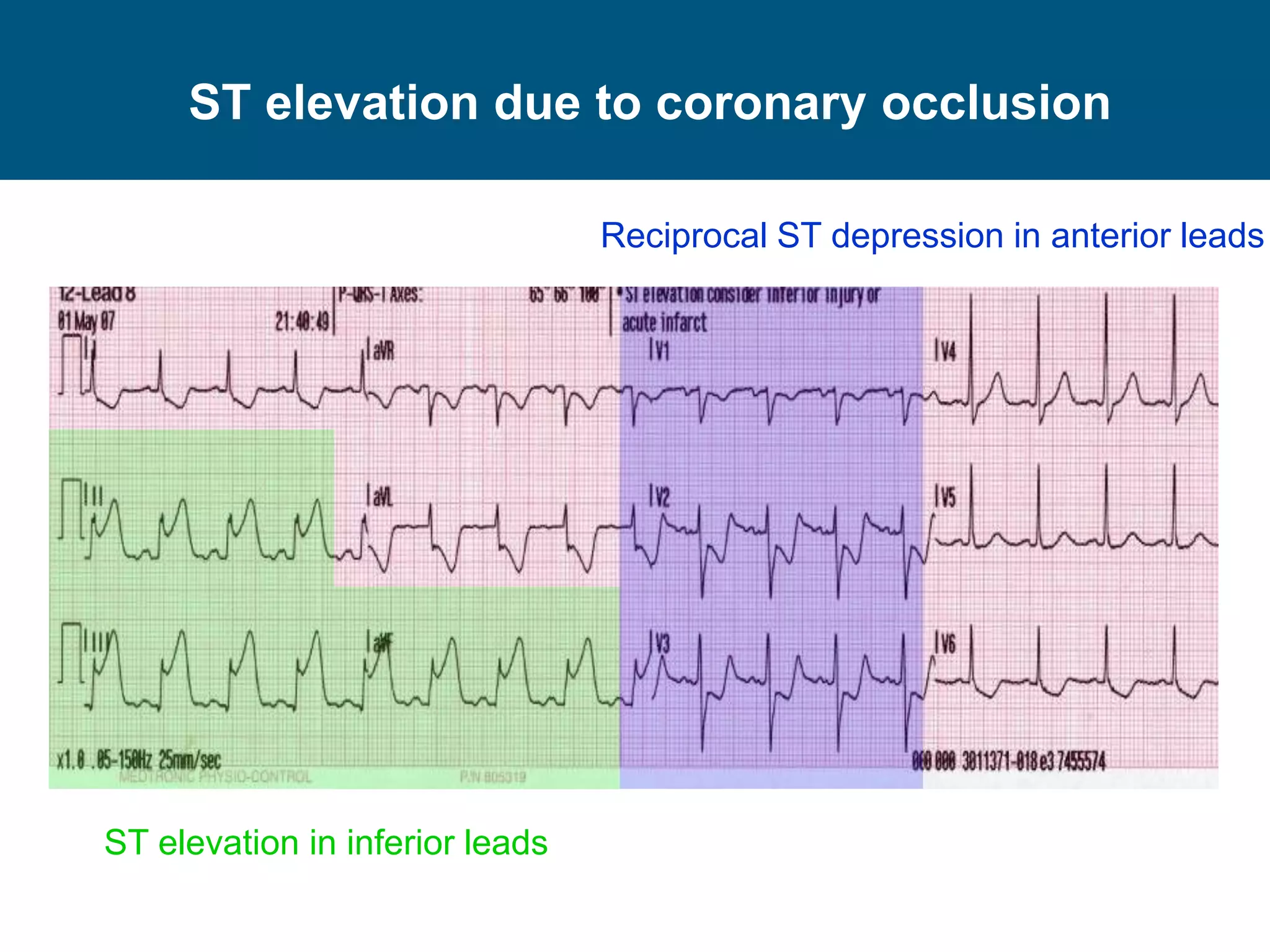

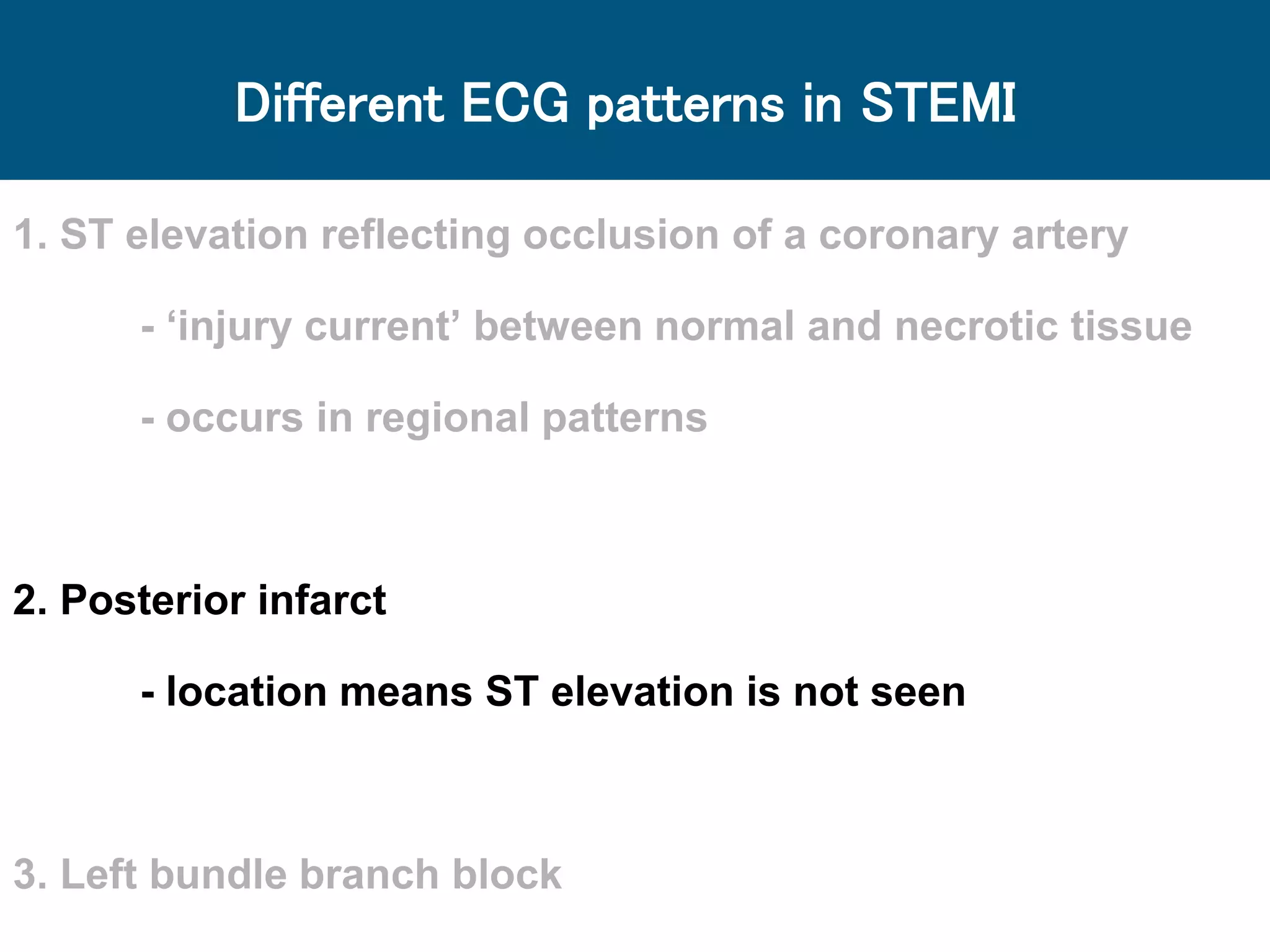
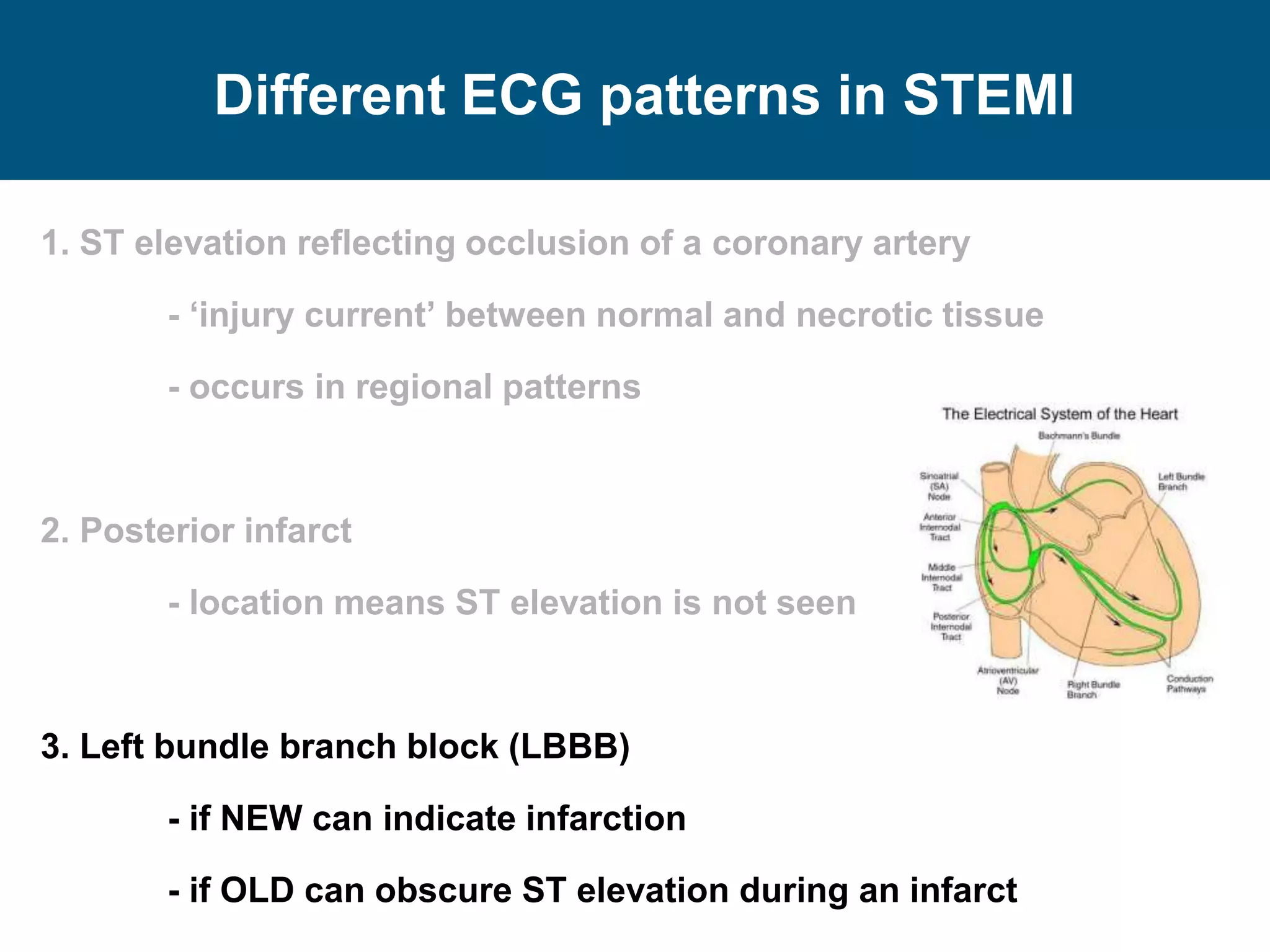



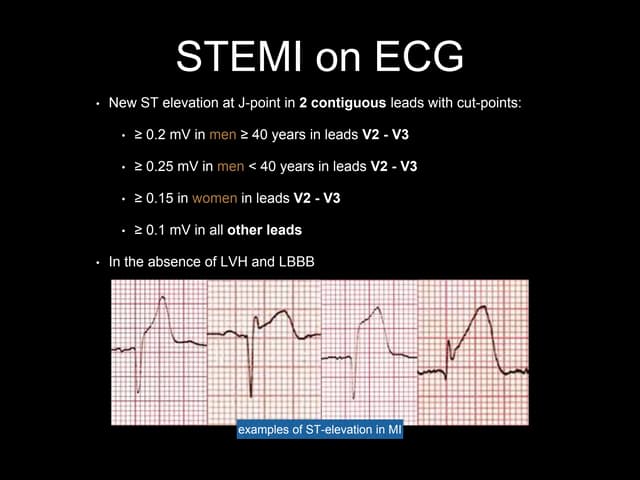
The document discusses ECG interpretation focusing on STEMI, its patterns, and the significance of rapid recognition for effective treatment. It outlines different ECG abnormalities associated with STEMI, including ST elevation indicating coronary artery occlusion and variations seen in left bundle branch blocks and posterior infarcts. The key takeaway is the importance of assessing clinical presentation and ECG details to minimize misdiagnosis and improve patient outcomes.