Downloaded 43 times



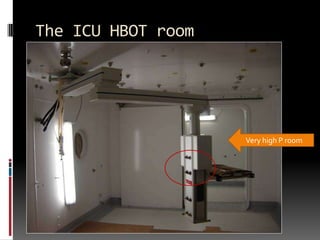
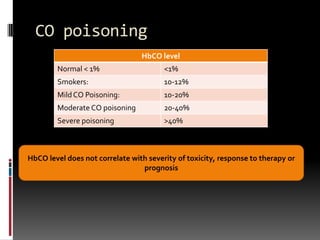
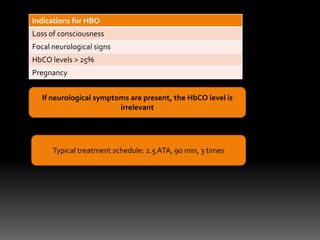

The document discusses the principles and applications of hyperbaric oxygen therapy (HBOT) in intensive care, covering topics such as gas laws, indications for use, and the differences between monoplace and multiplace chambers. It highlights key conditions treated with HBOT, including arterial gas embolism, necrotizing fasciitis, and carbon monoxide poisoning, while emphasizing the importance of early intervention and contraindications for the therapy. Practical considerations for patient transfer to HBOT units and potential side effects are also outlined.










































































