Downloaded 278 times
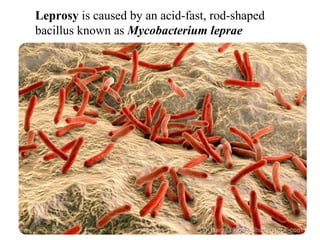
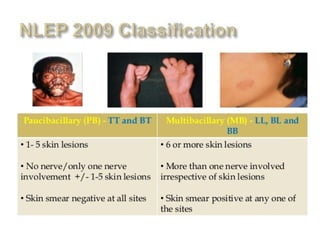
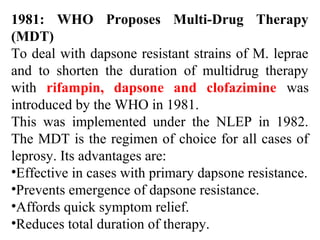
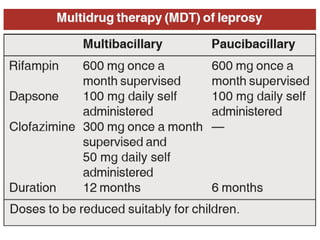
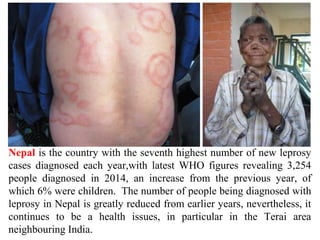



Leprosy is caused by Mycobacterium leprae and M. lepromatosis bacteria, which mainly affect the skin, mucus membranes, and nerves. It is classified based on the Ridley-Jopling system and can be paucibacillary or multibacillary. Leprosy is curable through multidrug therapy recommended by the WHO, which combines dapsone, rifampicin, and clofazimine. Nepal still has a significant number of new leprosy cases each year, particularly in the Terai region bordering India, though rates have decreased overall.








![Anthelmintic.[Pharmacology]](https://cdn.slidesharecdn.com/ss_thumbnails/anthelmintic-200607092955-thumbnail.jpg?width=640&height=640&fit=bounds)



































![7...Anti-leprotic drugs. [downloaded with 1stBrowser] (1)ggg (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/7-240830121631-79846044-thumbnail.jpg?width=640&height=640&fit=bounds)































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










