

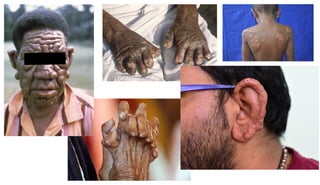
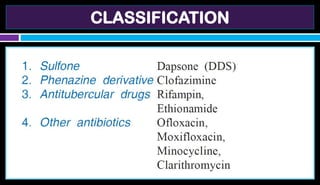
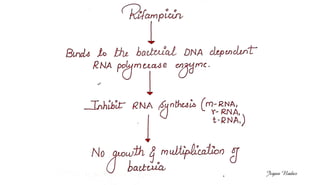


The document discusses leprosy, a contagious disease caused by Mycobacterium leprae that is now curable due to effective antileprotic drugs like dapsone and clofazimine. It highlights the mechanisms, uses, side effects, and resistance issues associated with these medications, emphasizing the importance of multidrug therapy. Additionally, it provides information on rifampin, an antitubercular drug, noting its absorption, metabolism, and common side effects.























































































