Diseases of the orbit
•Download as PPTX, PDF•
6 likes•2,274 views

This document discusses diseases of the orbit, including its anatomy and contents. It describes several common orbital conditions: - Orbital cellulitis is an acute infection behind the orbital septum that can lead to abscesses or complications like cavernous sinus thrombosis if not treated promptly with antibiotics. - Cavernous sinus thrombosis is a serious infection of the veins around the eye that can cause vision loss and nerve palsies if the infection spreads. It requires intensive IV antibiotics. - Thyroid eye disease is an autoimmune condition associated with Graves' disease where the muscles and fat behind the eye become inflamed, causing proptosis, eye movement issues, and eyelid changes. It is classified based

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Diseases of the orbit
Similar to Diseases of the orbit (20)
More from Bipin Bista
More from Bipin Bista (20)
Recently uploaded
Recently uploaded (20)
Diseases of the orbit
- 1. DISEASES OF THE ORBIT BIPIN BISTA OPHTHALMOLOGY RESIDENT, NMCTH
- 2. DISCUSSION Orbit Content Superior orbital fissure : structures Inferior O F Proptosis Pre—septal cellulitis Orbital cellulitis Cavernous sinus thrombosis Thyroid Ophthalmopathy
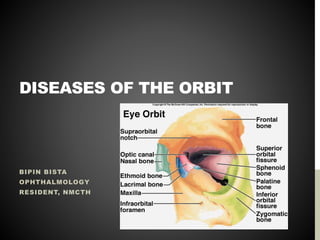
- 3. ORBIT Quadrangular pyramids situated between the anterior cranial fossa and the maxillary sinuses below. 40 mm in height, width and depth Formed by 7 seven bones : Frontal, Maxilla, Zygomatic, Sphenoid, Palatine, Ethmoid and Lacrimal. Has 4 walls – medial, lateral, superior and inferior.
- 4. WALLS OF ORBIT Medial – 2 orbits are parallel , common for #. Inferior – (floor) triangular , commonly involved in blow—out #. Lateral – triangular, covers posterior half. Roof – formed by orbital plate of frontal bone. Apex – posterior end where 4 walls converge , 2 orifices, the optic canal which transmits optic nerve and ophthalmic artery and Superior orbital fissure which transmits arteries, veins and nerves.
- 5. FASCIA BULBI (TENON’S CAPSULE) Envelops the globe from the margin of cornea to the optic nerve. It has thickened lower part to form a sling where the globe rests ; ‘Suspensory ligament of Lockwood’ .
- 6. CONTENTS OF ORBIT Volume : 30 cc. 1/5th is occupied by eyeball. Part of optic nerve, Extraocular muscles , lacrimal gland, lacrimal sac, ophthalmic artery and its branches, 3rd, 4th and 6th cranial nerves and ophthalmic & maxillary divisions of cranial nerves , sympathetic nerve and fascia.
- 7. SUPERIOR ORBITAL FISSURE It is a foramen in skull lying between lesser and greater wing of sphenoid.
- 8. STRUCTURES PASSING THROUGH SOF Superior and inferior division of Oculomotor nerve.(3) Trochear nerve(4) Lacrimal, frontal and nasociliary nerve of Ophthalmic branch of Trigeminal nerve (V1)(5) Abducent nerve (6) Superior and inferior division of Ophthalmic vein Sympathetic fibers from cavernous plexus.
- 9. INFERIOR ORBITAL FISSURE Zygomatic branch of trigeminal nerve and ascending branch of pterygopalatine ganglion
- 10. PROPTOSIS Forward displacement of eyeball beyond orbital margins. Classification : 1. Unilateral 2. Bilateral 3. Acute 4. Intermittent 5. Pulsating
- 11. UNILATERAL PROPTOSIS Congenital : dermoid, teratoma Trauma : Orbital hemorrhage, FB, aneurysm, emphysema Inflammatory : cellulitis, thrombophlebitis, CST, Panophthalmitis. Circulatory : varix and aneurysms Cysts : hydatid cyst, cysticercus Tumours : primary, secondary or metastatic Mucoceles of PNS : Common – frontal , ethmoidal and maxillary.
- 12. BILATERAL PROPTOSIS • Developmental anomalies : Craniofacial dysostosis • Osteopathies : Rickets, acromegaly • Inflammatory condition : Mikulicz’s disease, CST • Endocrinal exophthalmos : Thyroid ds • Tumors : Lymphoma, lymphosarcoma • Systemic disease : Histiocytosis,amyloidosis
- 13. ACUTE PROPTOSIS EXTREME RAPIDITY • Orbital emphysema • Orbital hemorrhage • Rupture of ethmoidal mucocele
- 14. INTERMITTENT PROPTOSIS On/Off , • Orbital varix • Periodic orbital oedema • Recurrent orbital hemorrhage • Vascular tumors
- 15. PULSATILE PROPTOSIS Caroticocavernous fistula Saccular aneurysm of Ophthalmic artery Deficient Orbital floor
- 16. INVESTIGATION History Local examination • Inspection • Palpation • Auscultation • Transillumination • Visual acuity • Pupil reaction • Fundoscopy • Ocular motility • Exophthalmometry • Perimetry Systemic examination Laboratory investigation Imaging Invasive procedure – Orbital venography, carotid angiography, radioisotope arteriography. Histopathological
- 18. PRESEPTAL CELLULITIS Infection of subcutaneous tissues anterior to the orbital septum. Causes : Staphylococcus aureus or Streptococcus pyogenes, occassionally Haemophilus influenza.
- 20. CLINICAL FEATURES Inflammatory oedema of lids and periorbital skin sparing the orbit. Painful periorbital swelling Erythema & hyperaemia of lids Fever & leucocytosis Proptosis – absent Normal ocular movements Conjunctiva- not congested VA – Normal
- 21. TREATMENT Systemic antibiotics › Mild to Moderate : Oral co-amoxiclav 500/125 mg tds or Clox 500 mg QID for about 10 days. › Severe : IV Ceftriaxone 1-2 g/day in divided dose for 4-5 days. › Systemic analgesics › Warm compression › Surgical exploration
- 22. ORBITAL CELLULITIS Acute infection of orbital tissues of the orbit behind the orbital septum. May or may not develop to subperiosteal abscess or orbital abscess. Pathology : similar to suppurative inflammation of body in general. • Infection establishes early d/t absence of lymphatics • Rapid spread with extensive necrosis • Raised IOP d/t tight compartment.
- 23. CLINICAL FEATURES • SYMPTOMS Swelling & severe pain . Associated general symptoms Vision loss &/or diplopia • SIGNS Swelling of lids Chemosis of conjunctiva Axial proptosis Restricted ocular movements RAPD Papillitis or Papilloedema
- 24. COMPLICATIONS Ocular : Exposure keratopathy, optic neuritis and CRAO. Orbital : Subperiosteal abscess &/or orbital abscess. Temporal/parotid abscess Intracranial complication : CST, Meningitis & Brain Abscess. Septicaemia & pyaemia.
- 25. INVESTIGATIONS Bacterial cultures Complete haemogram X-ray : PNS Orbital USG CT scan & MRI
- 26. TREATMENT Intensive antibiotic therapy Analgesic & anti-inflammatory Topical antibiotics Nasal decongestant Revaluation Surgical intervention : canthotomy/cantholysis
- 27. CAVERNOUS SINUS THROMBOSIS Septic thrombosis of cavernous sinus is a disastrous sequela, resulting from spread of sepsis travelling along the tributaries from the infected sinuses, teeth, ears, nose, and skin of the face.
- 28. COMMUNICATIONS Anteriorly : superior and inferior ophthalmic vein drain in the sinus. Receive blood from face, nose, pns & orbits. Posteriorly : Superior and inferior petrosal sinuses leave it to join lateral sinus. Labyrinthine vein opening into inferior petrosal sinuses Superiorly : veins of cerebrum and may be infected from meningitis and cerebral abscesses. Inferiorly : pterygoid venous plexus Medially : transverse sinus which connects two cavernous sinuses.
- 29. CLINICAL FEATURES Usually starts unilateral condition , which soon becomes bilateral in more than 50% of cases d/t intercavernous communication General features : severe, high grade fever chills and rigor , vomiting & headache.
- 30. OCULAR FEATURES Severe pain in the eye and forehead on the affected side Conjunctiva is swollen and congested. Proptosis develops rapidly Ipsilateral ophthalmoplegia – Diplopia caused d/t palsy of 3rd, 4th and 6th cranial nerves. Ipsilateral ptosis, dilated pupil, and absence of direct and consensual pupillary light reflex – 3rd nerve palsy. Corneal anaesthesia Oedema in the mastoid region. Fundus : may be normal, retinal vein may be congested.
- 31. INVESTIGATIONS Ct scan head MR venography Blood C/S
- 32. COMPLICATIONS Hyperpyrexia and signs of meningitis or pulmonary infarction.
- 34. THYROID EYE DISEASE Also labelled as : • Endocrine exophthalmos • Malignant exophthalmos • Dysthyroid ophthalmopathy • Graves disease • Thyroid associated ophthalmopathy
- 36. RISK FACTORS Females (4-6 times) common than male. Smoking Middle age Autoimmune thyroid disease HLA-DR3 & HLA-B8
- 37. PATHOGENESIS Autoimmune disease with orbital fibroblasts as the primary target of inflammatory attack and EOM being secondarily involved. Target antigen is shared between the thyroid follicular cells and orbital fibroblasts. Activated T—cell act on fibroblast-adipocyte lineage within the orbit and stimulate adipogenesis, fibroblast proliferation and glycosaminoglycan synthesis.
- 38. CLINICAL FEATURES 1. Lid signs • Dalrymple’s sign : retraction of the upper lids • Von Graefe’s sign : when globe is moved up, the globe lags behind. • Enroth’s sign : Fullness of eyelid. • Gifford’s sign: difficulty in eversion of eyelid • Stellwag’s sign : Infrequent blinking
- 39. C/F (CONTINUED) • Conjunctival signs : deep injection & chemosis. • Pupillary signs : less important – Ocular motility defects : Mobious sign – convergence weakness to partial or complete immobility of one or all EOM. – Unilateral elevator palsy :d/t IR failure – Failure of abduction due to MR involvement • Exophthalmos • Exposure keratitis • Optic neuropathy
- 40. CLASSIFICATION “NO SPECS” Class 0:N: No signs and symptoms Class 1:O: Only signs no symptoms(signs are limited to lid retraction,with or without lid lag and mild proptosis) Class 2:S: Soft tissue involvement with signs including lacrimation,photophobia,lid or conjunctival swelling Class 3:P: Proptosis is well established Class 4:E: Extraocular muscle involvement Class 5:C: Corneal involvement Class 6:S: Sight loss due to optic nerve involvement
- 41. CLINICAL COURSE • Self-limiting disease • Lasts from 1-5 years • Phases: 1. Congestive or active phase 2. Fibrotic or inactive phase
- 42. DIAGNOSIS 1. TFT 2. Thyroid Antibody Assay 3. USG 4. CT Scan 5. MRI
- 43. MANAGEMENT 1. Periodic clinical workup 2. Non-surgical measures 3. Surgical management
- 44. PERIODIC CLINICAL WORK UP Pain 1.Retrobulbar pain 2.Pain on ocular movement Redness 3.Redness of lids 4.rednesss of conjunctiva Swelling 5.swelling of lids 6. swelling of conjunctiva 7. swelling of caruncle 8.proptosis(≥ 𝟐𝐦𝐦 𝐢𝐧𝐜𝐫𝐞𝐚𝐬𝐞 in proptosis over 1-3 months) Loss of function 9.Decrease in eye movement by ±𝟓 𝐝𝐞𝐠𝐫𝐞𝐞 𝐨𝐯𝐞𝐫 𝟏 − 𝟑 𝐦𝐨𝐧𝐭𝐡𝐬 10.Decrease vision by ≥ 1 snellen line over 1-3 months Ocular motility work up:Binocular,uniocular,VFA
- 45. NON-SURGICAL MANAGEMENT 1. Smoking cessation 2. Head elevation at night and cold compress in morning 3. Lubricating artificial tear drops 4. Eyelid taping 5. Guanethidine 5% eyedrops 6. Prisms 7. Systemic steroids 8. Radio therapy 9. Combined therapy
- 46. SURGICAL MANAGEMENT 1. Orbital decompression 2. Extra-ocular muscle surgery 3. Eyelid surgery
- 47. THANK YOU