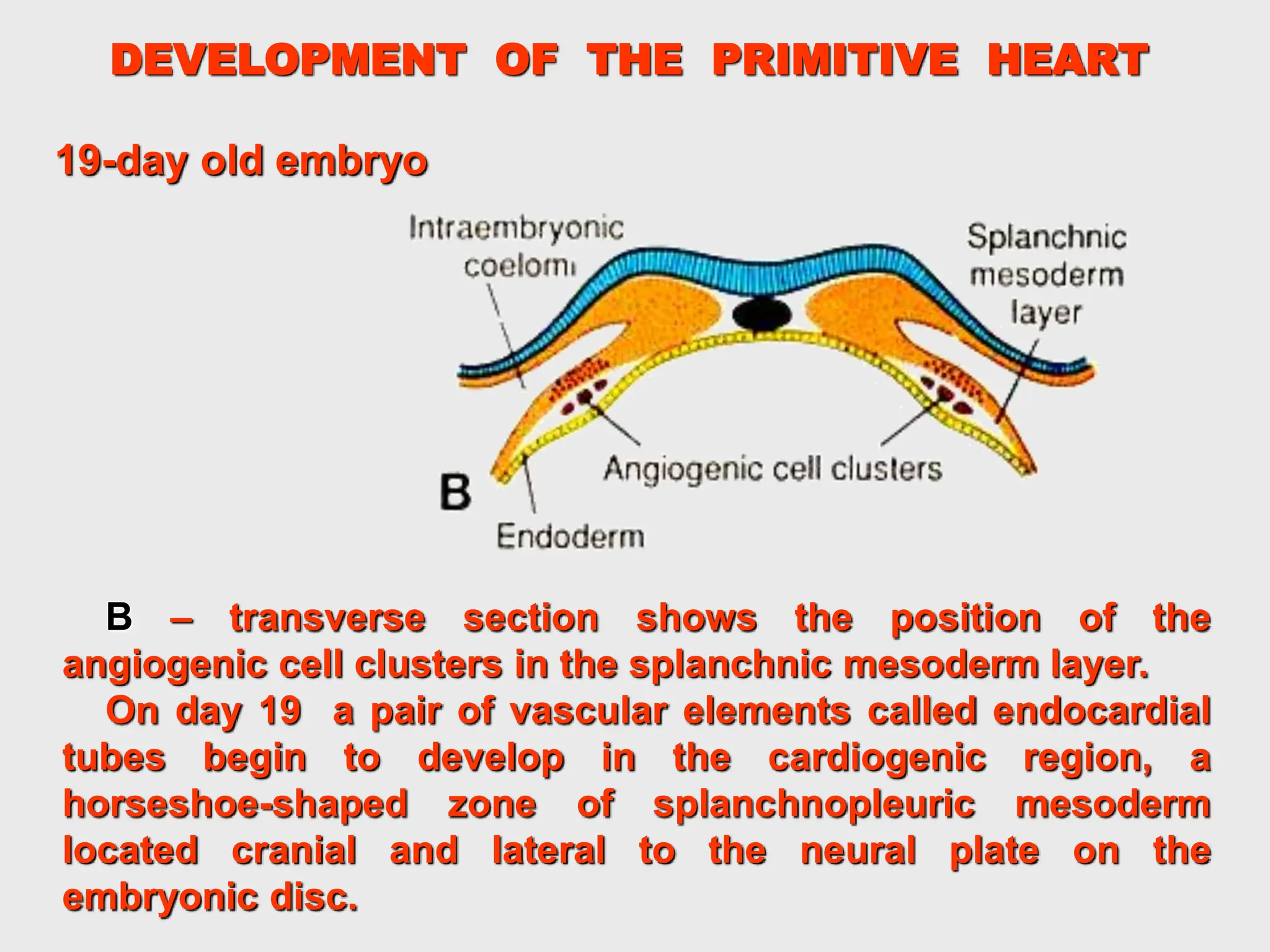
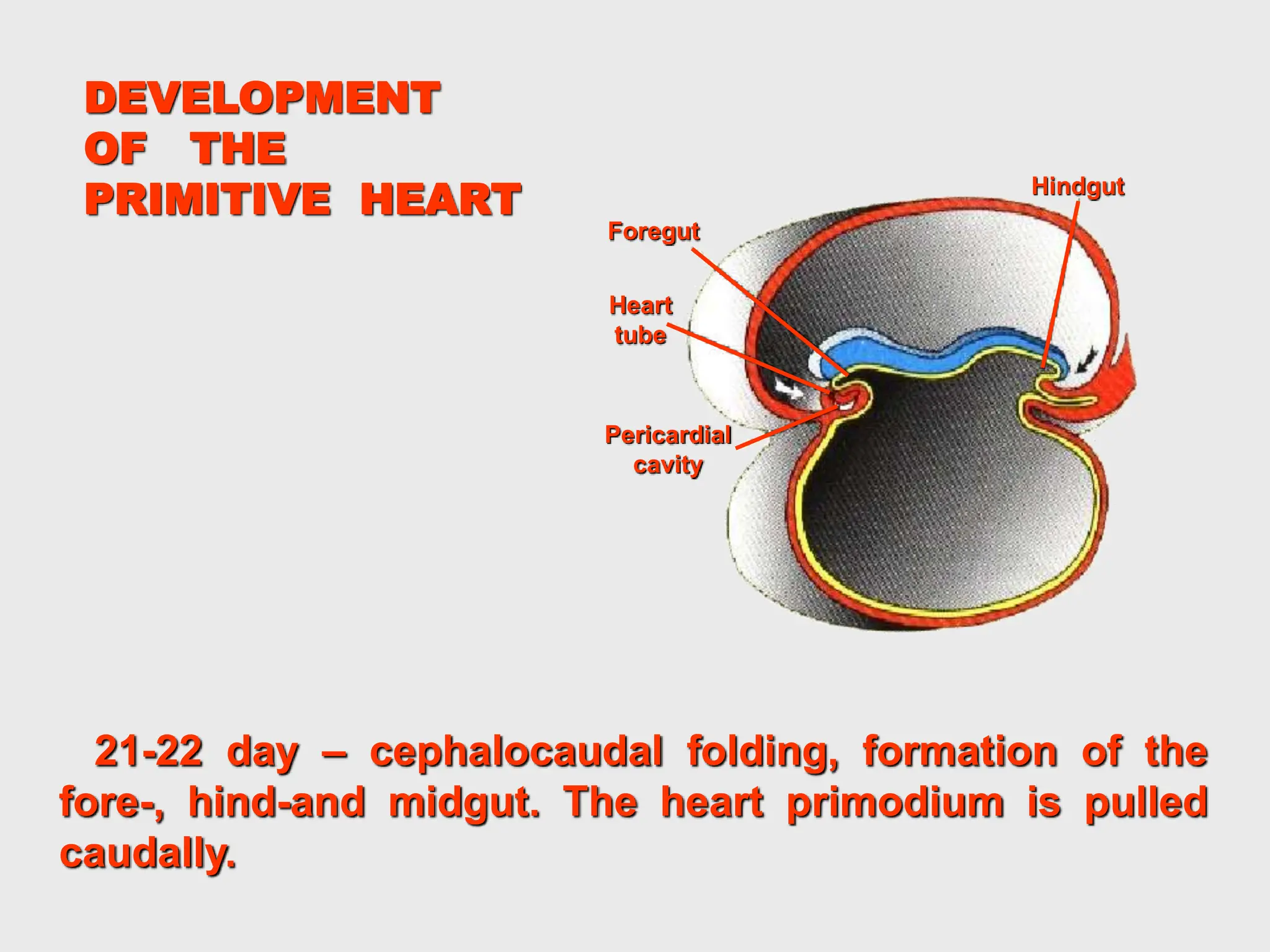
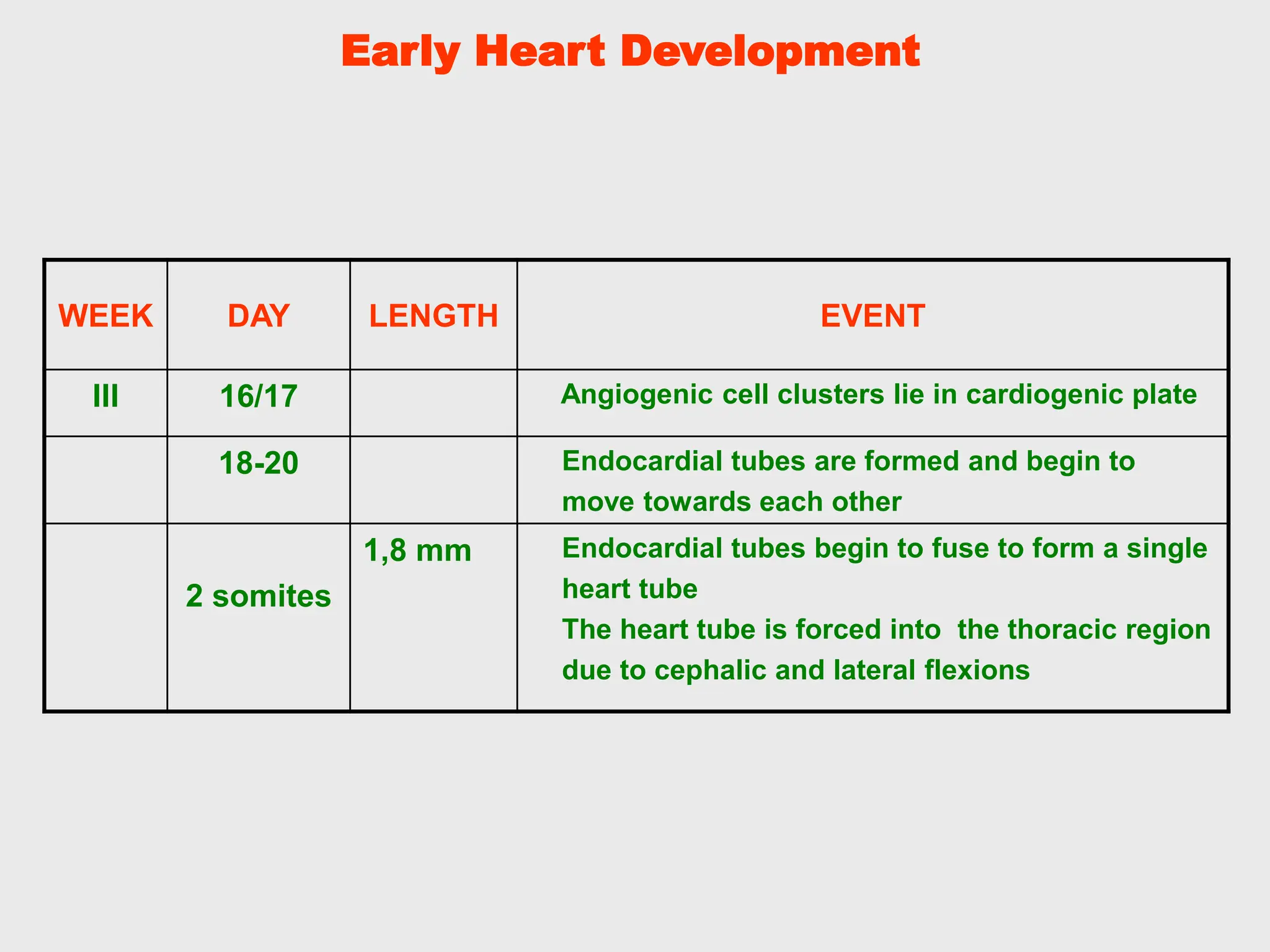
The document describes the early development of the heart in an embryo. It begins with angiogenic cell clusters in the cardiogenic area that form endocardial tubes on day 19. These tubes fuse to form a single endocardial tube by day 21. The tube develops constrictions that outline the bulbus cordis, truncus arteriosus, primitive ventricle, and primitive atria. By day 22, the heart starts beating ineffectively. Circulation begins between days 27-29 as the heart further develops structures like the atrioventricular canal. The document provides detailed information on heart development from approximately days 16-40 of embryogenesis.