The document describes the development of the cardiovascular system in three main stages:
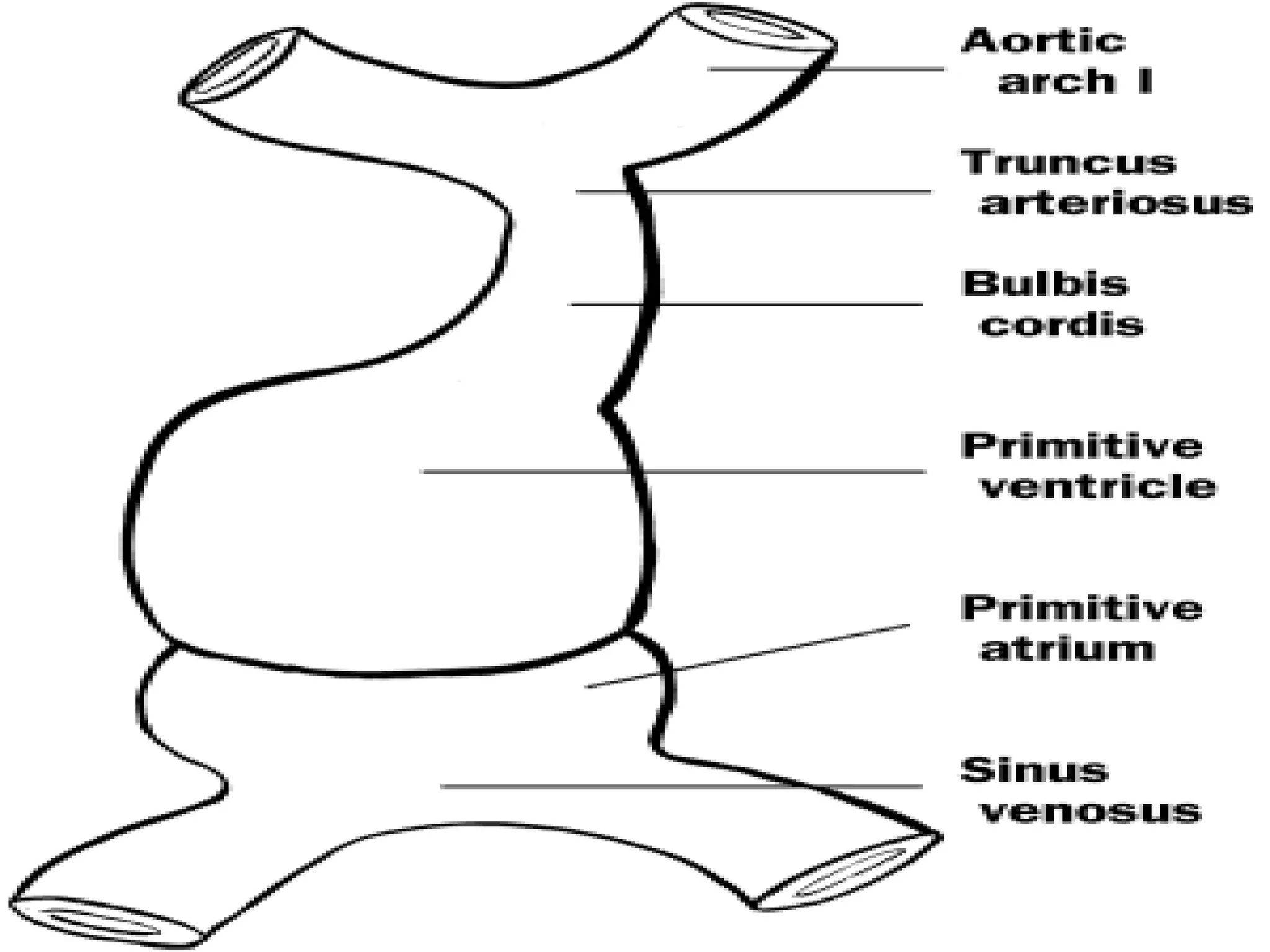
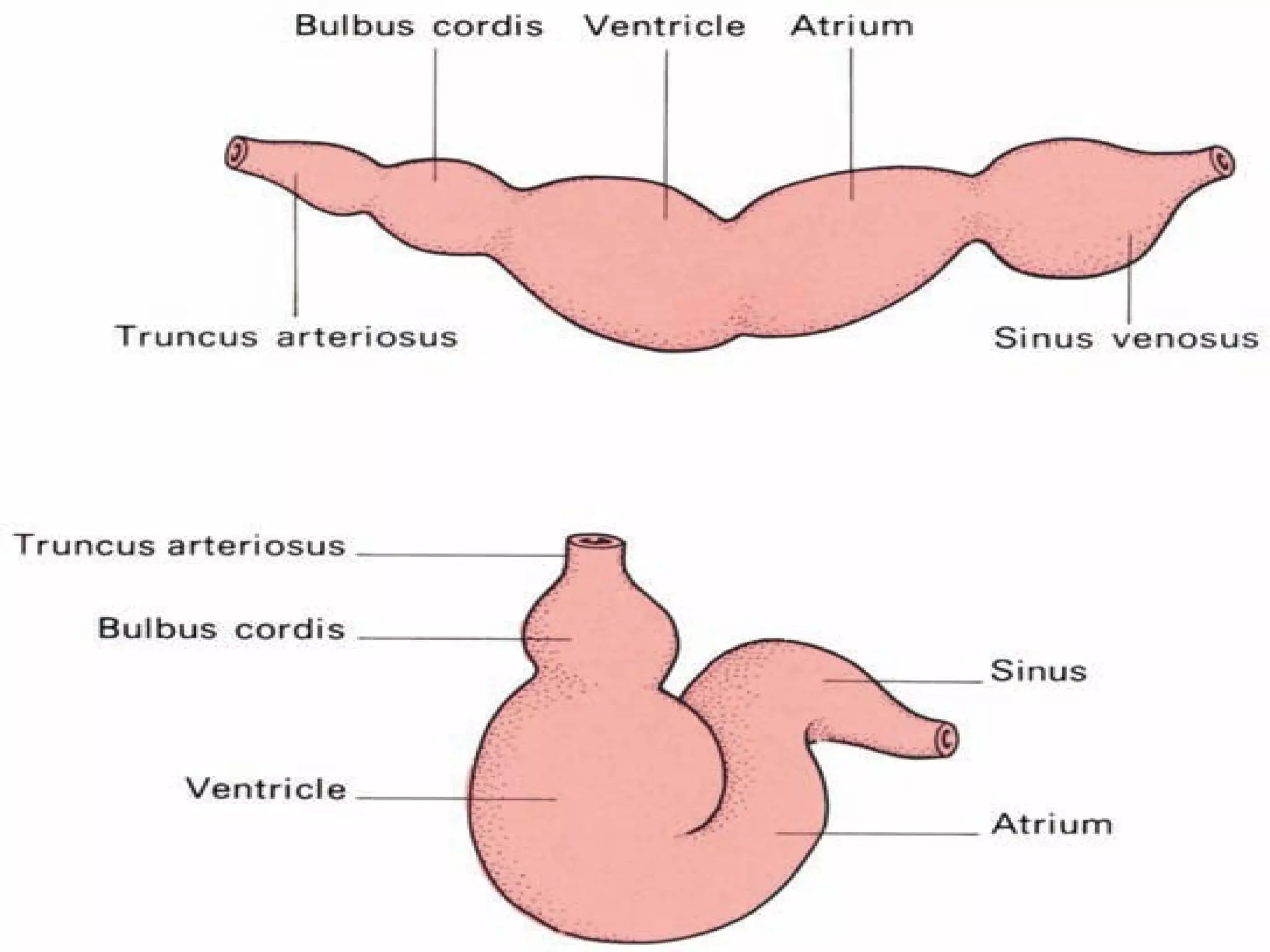
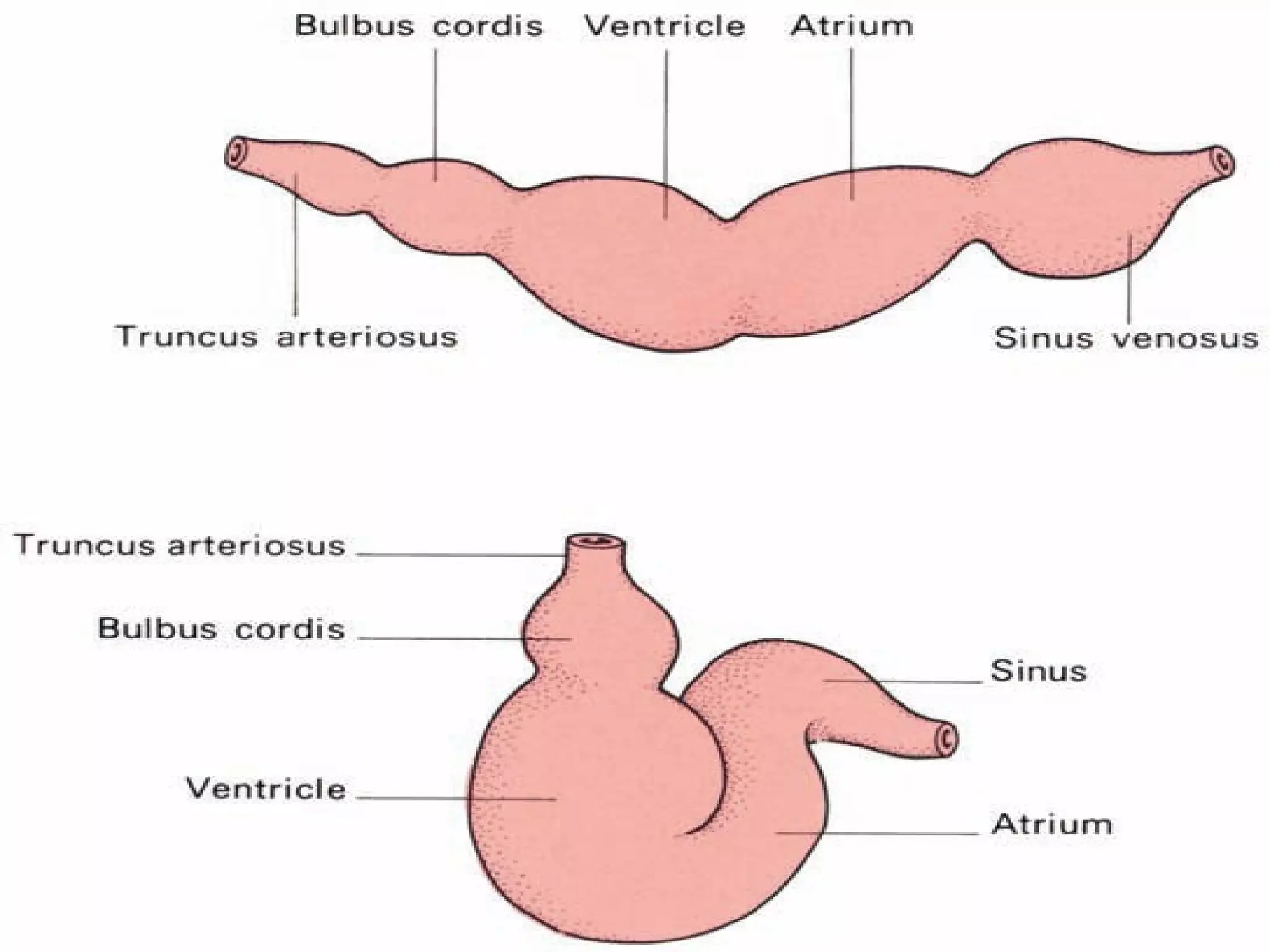
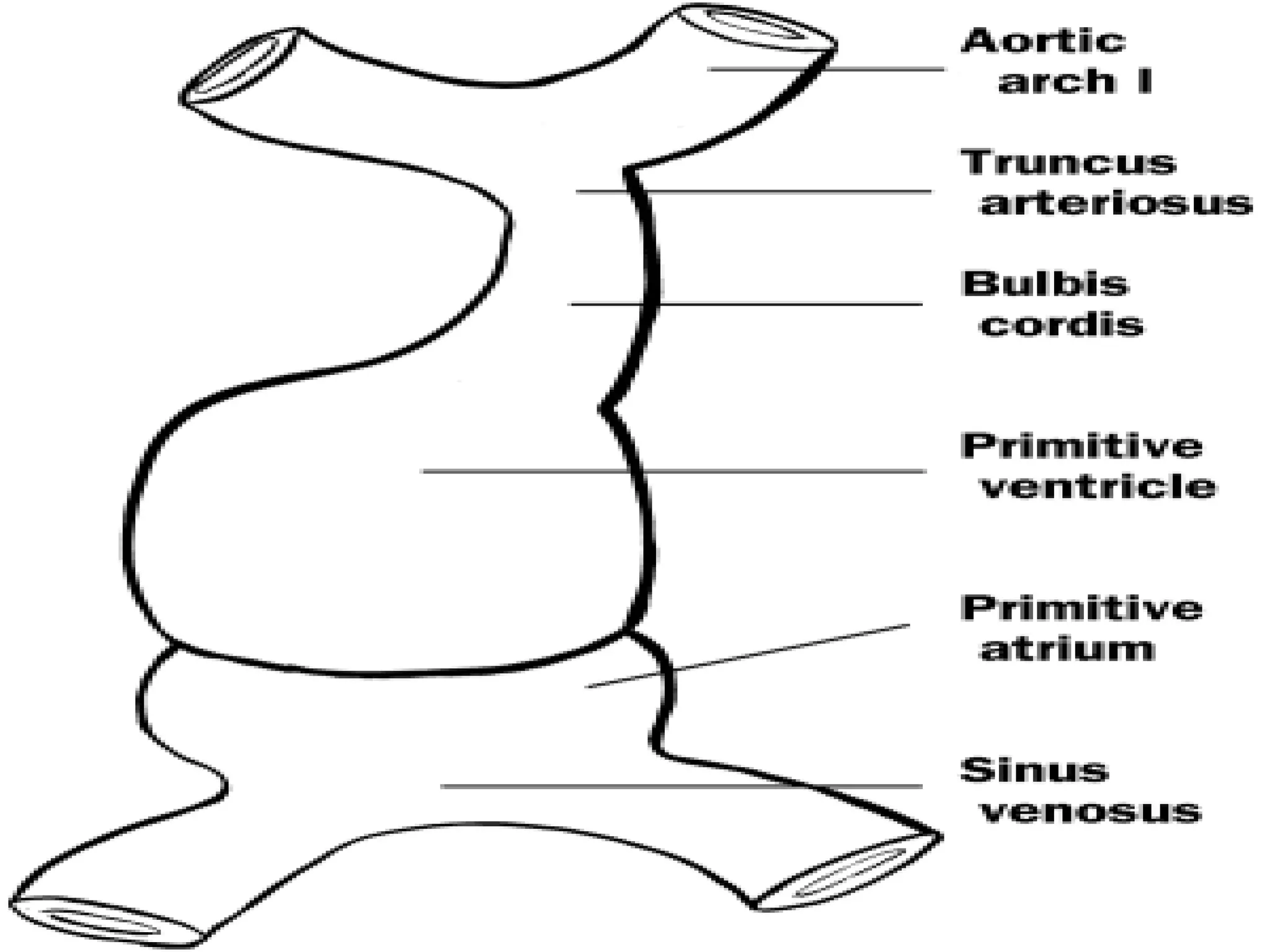
1. The formation of the primitive heart tube from angioblastic cords that fuse to form a single tube.
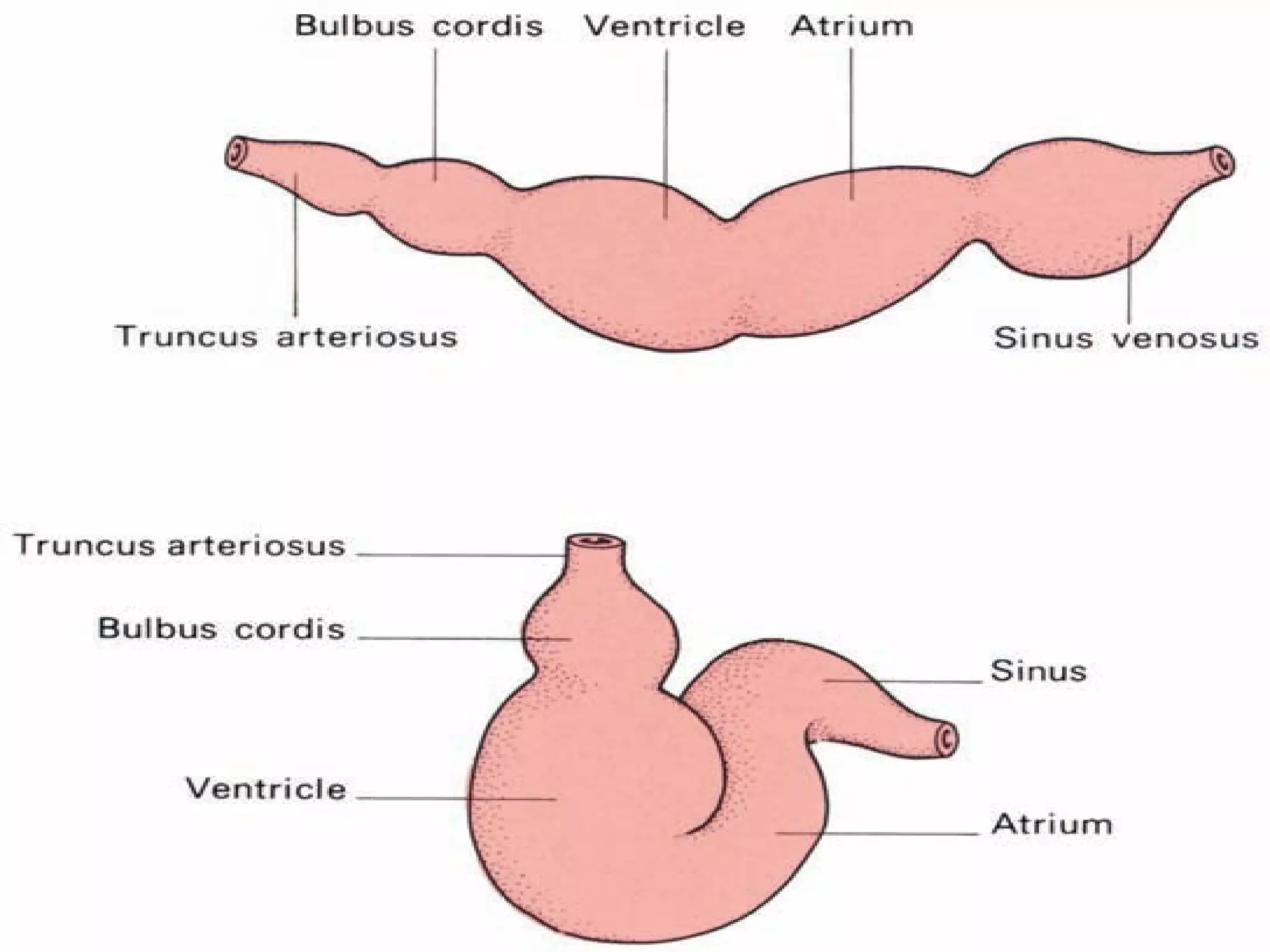
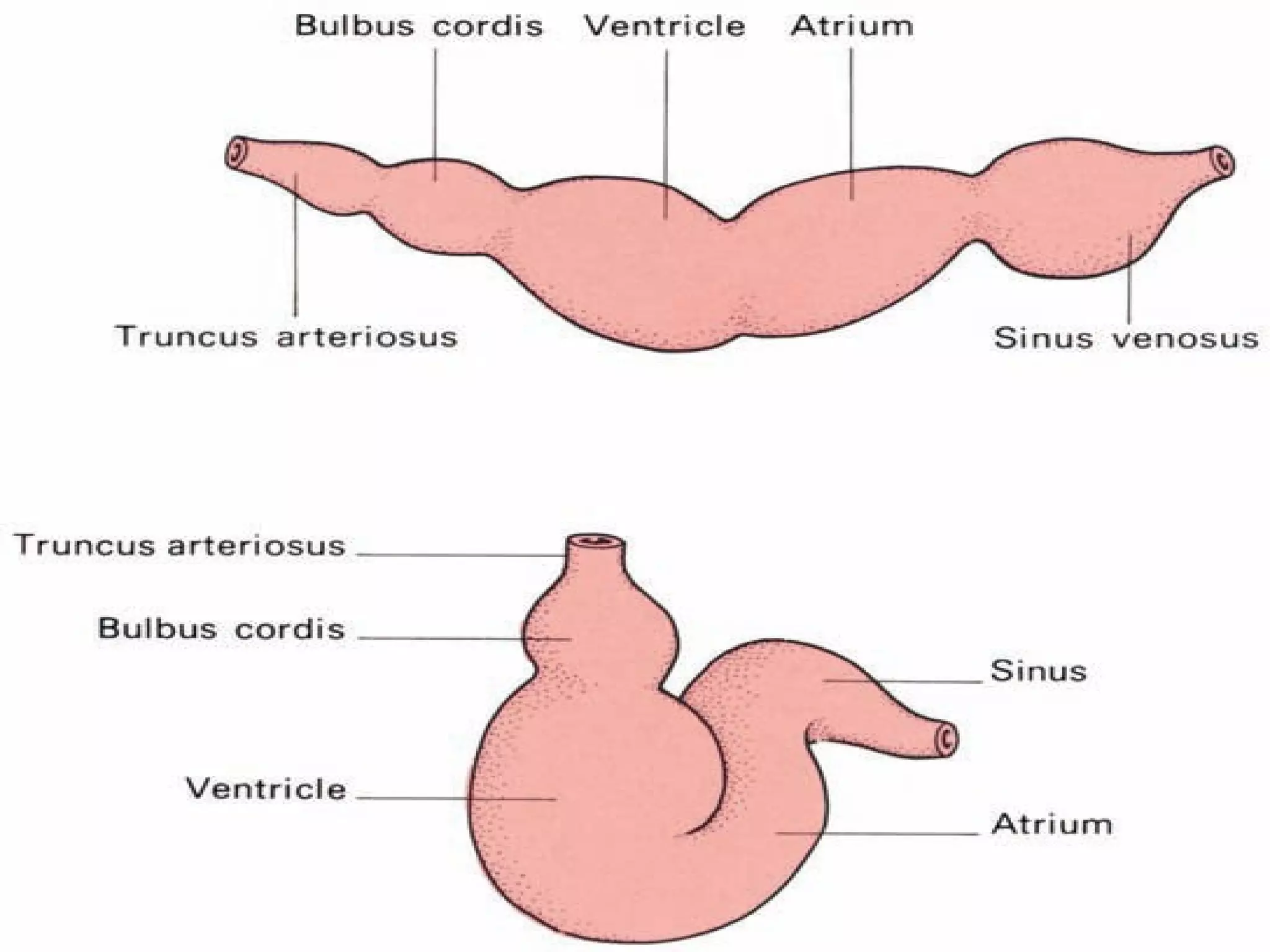
2. Looping and folding of the heart tube into a U-shape as the head folds, dividing it into chambers.
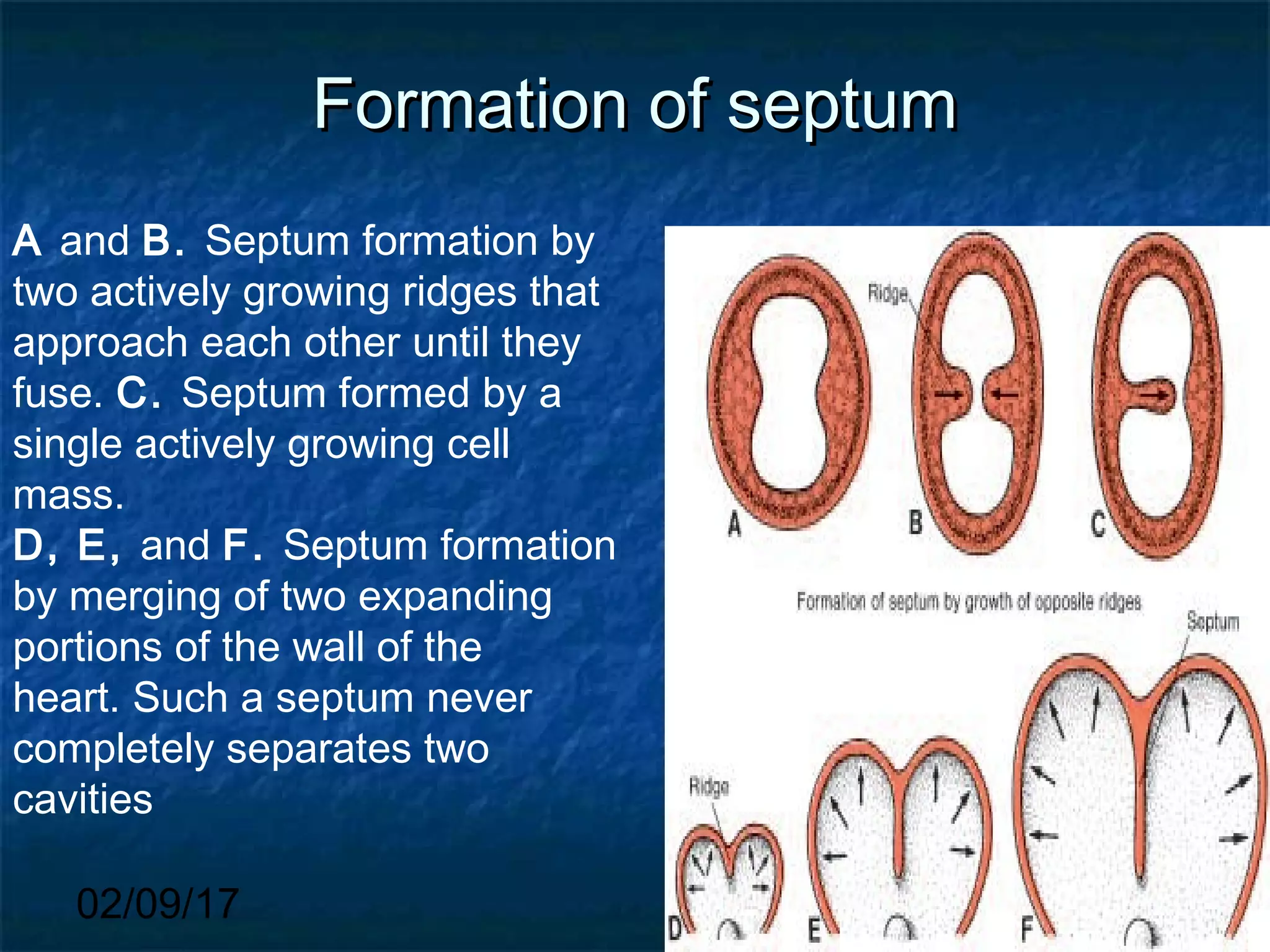
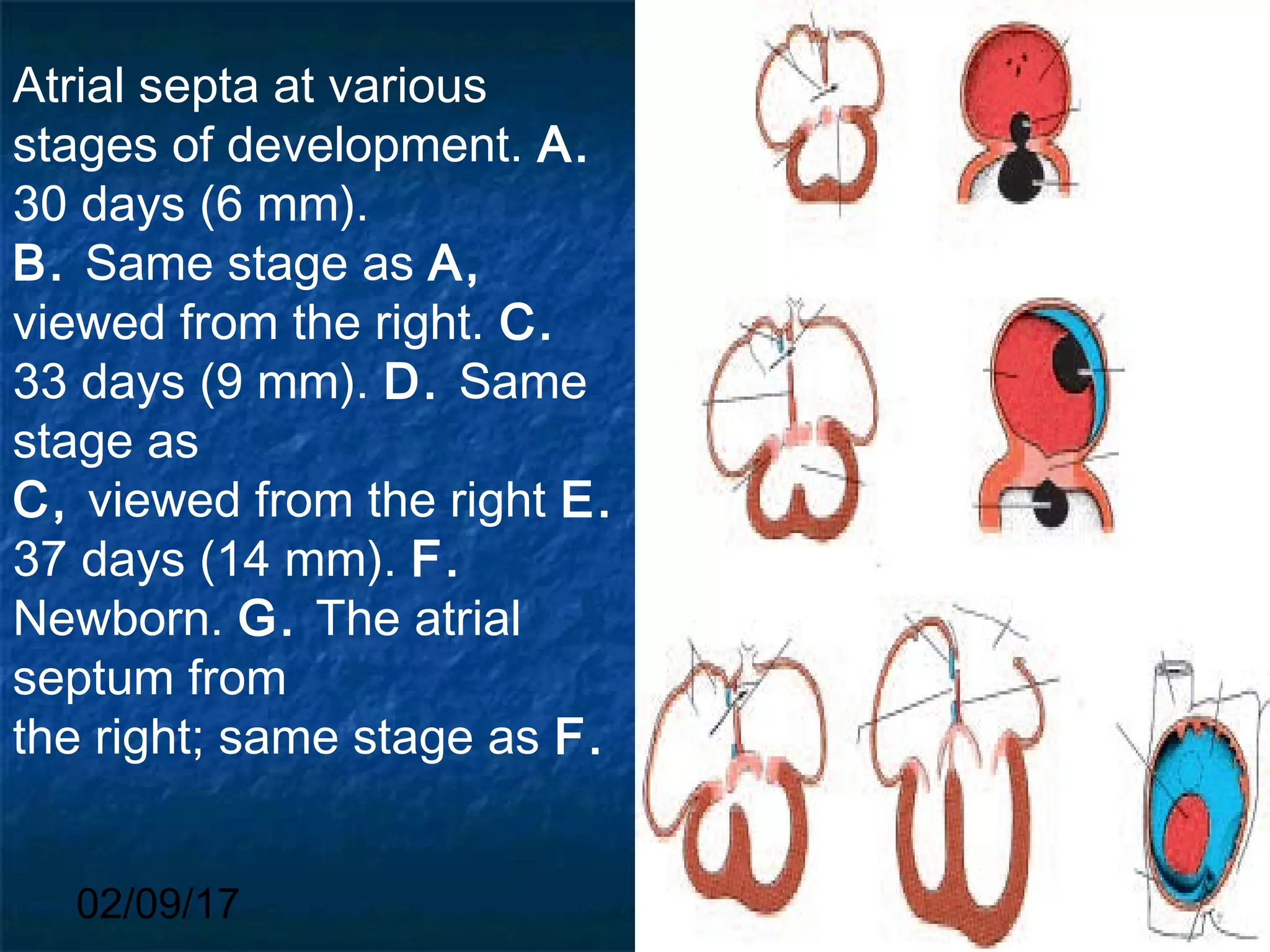
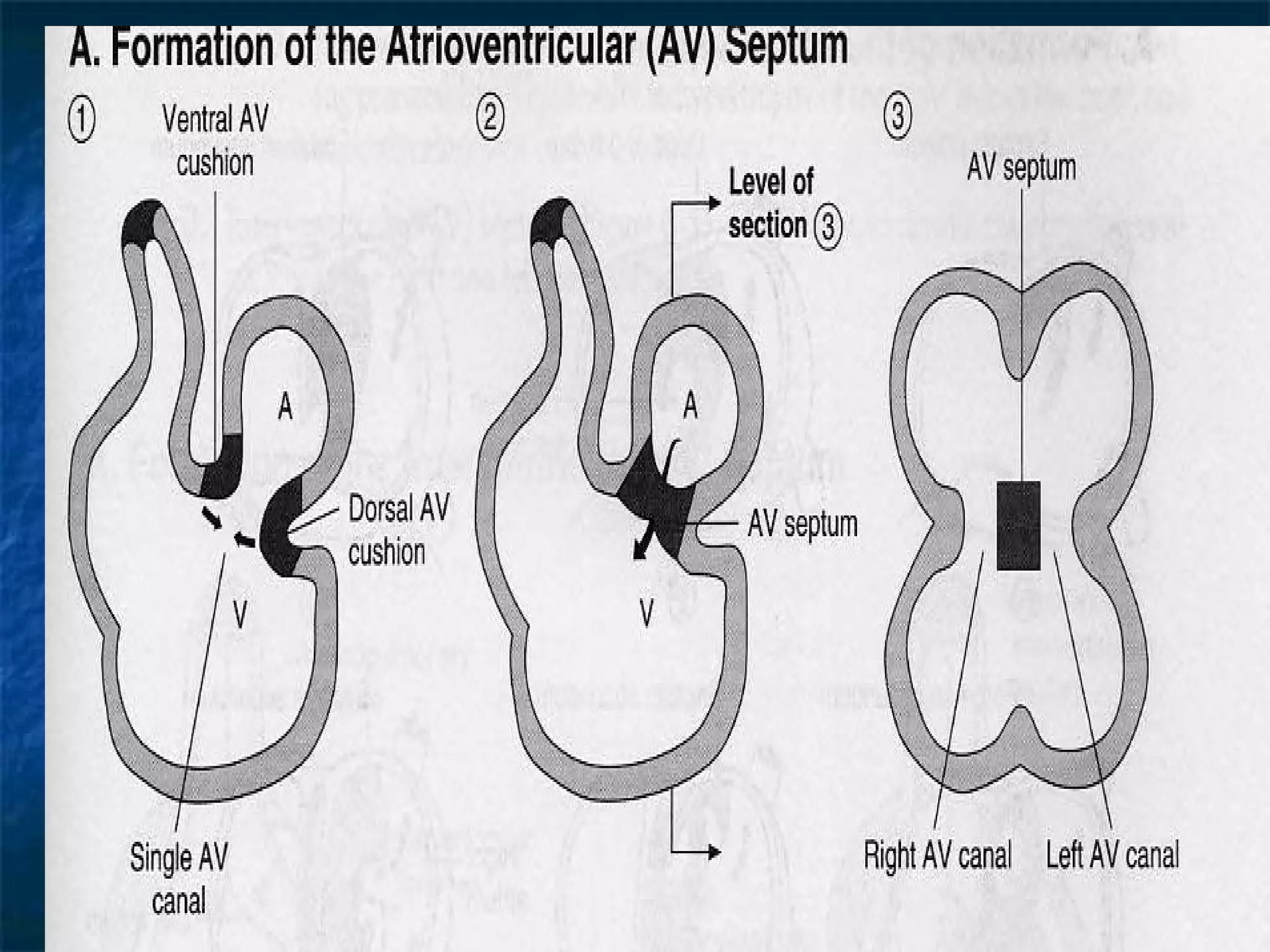
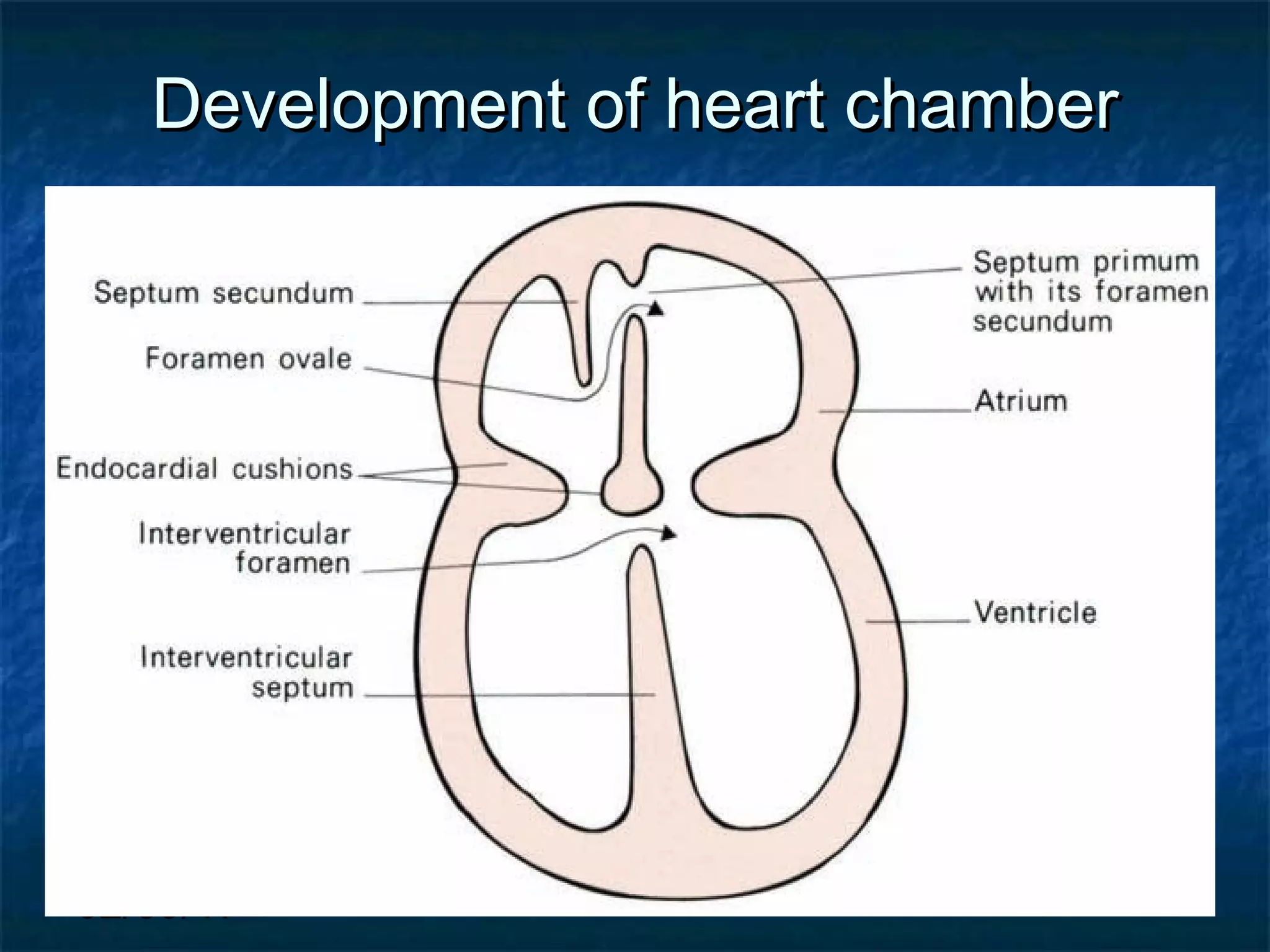
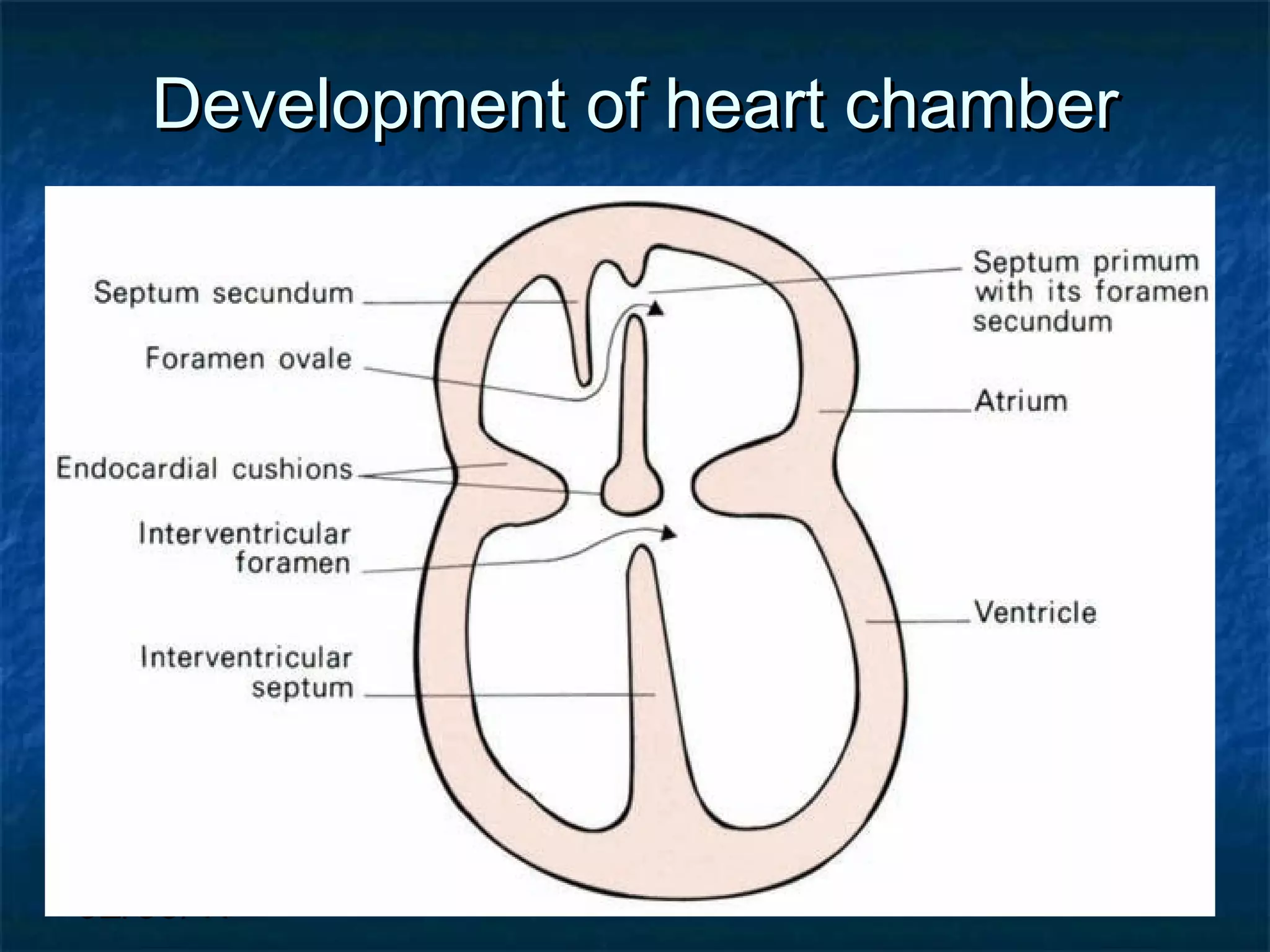
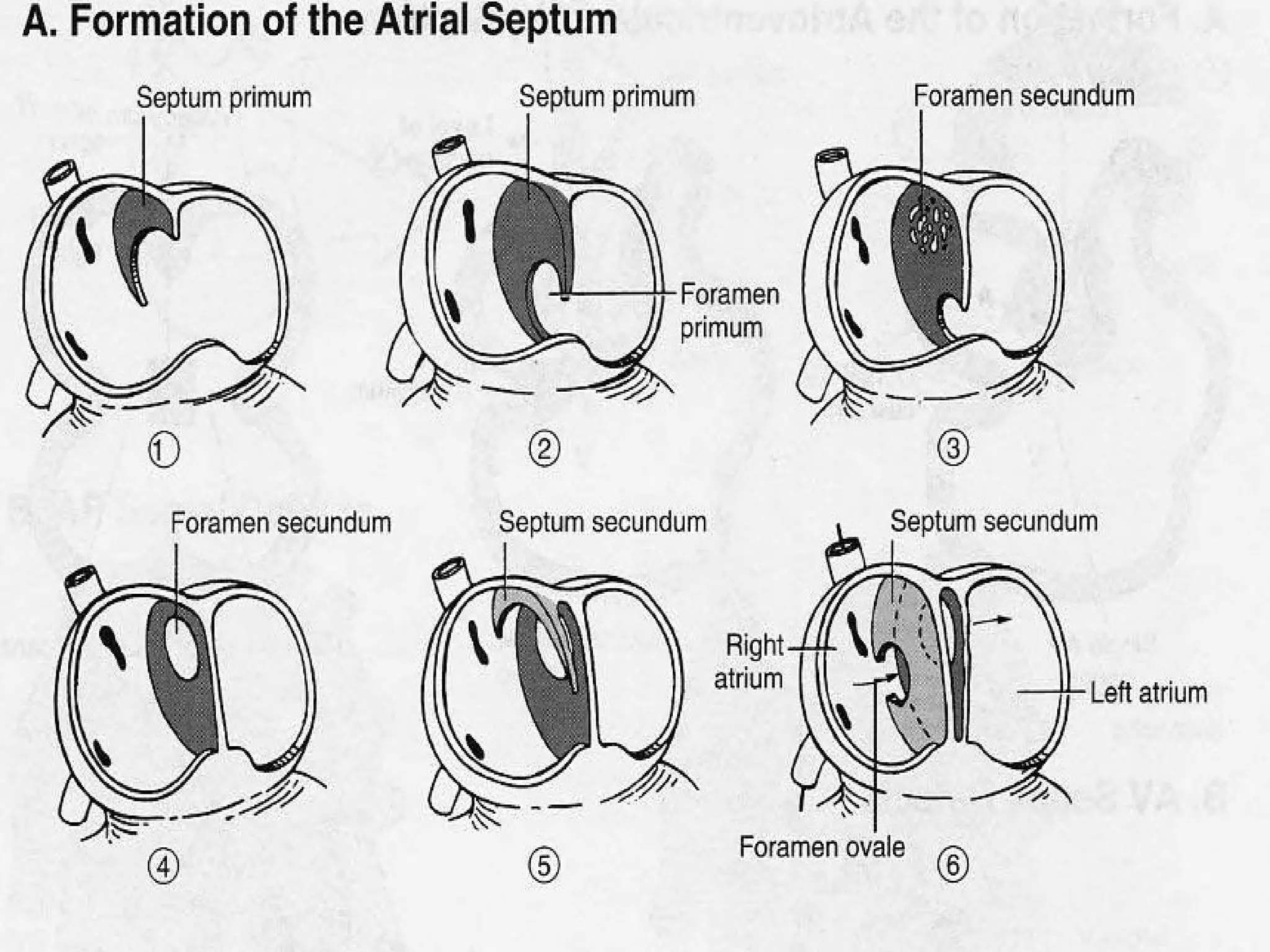
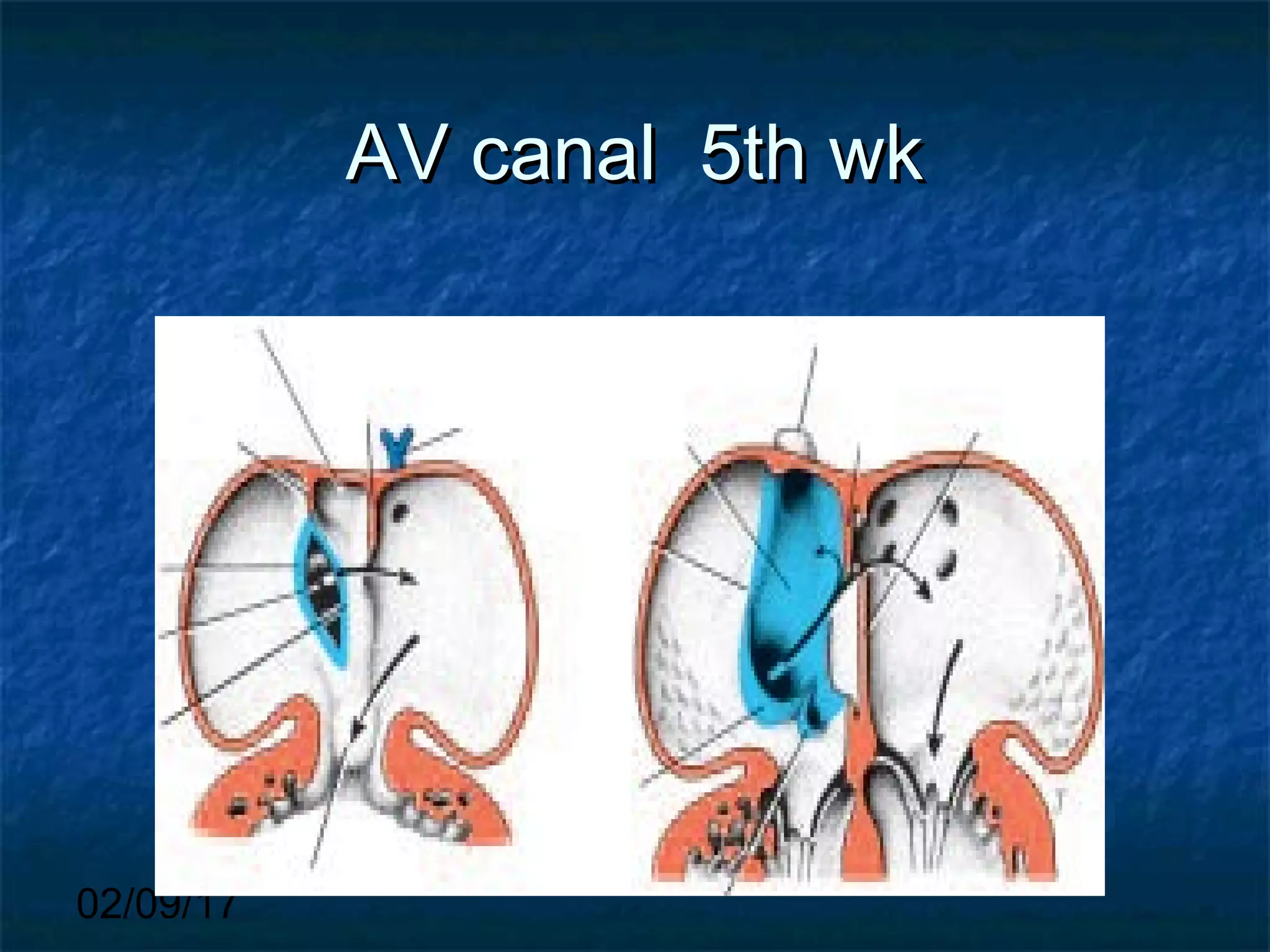
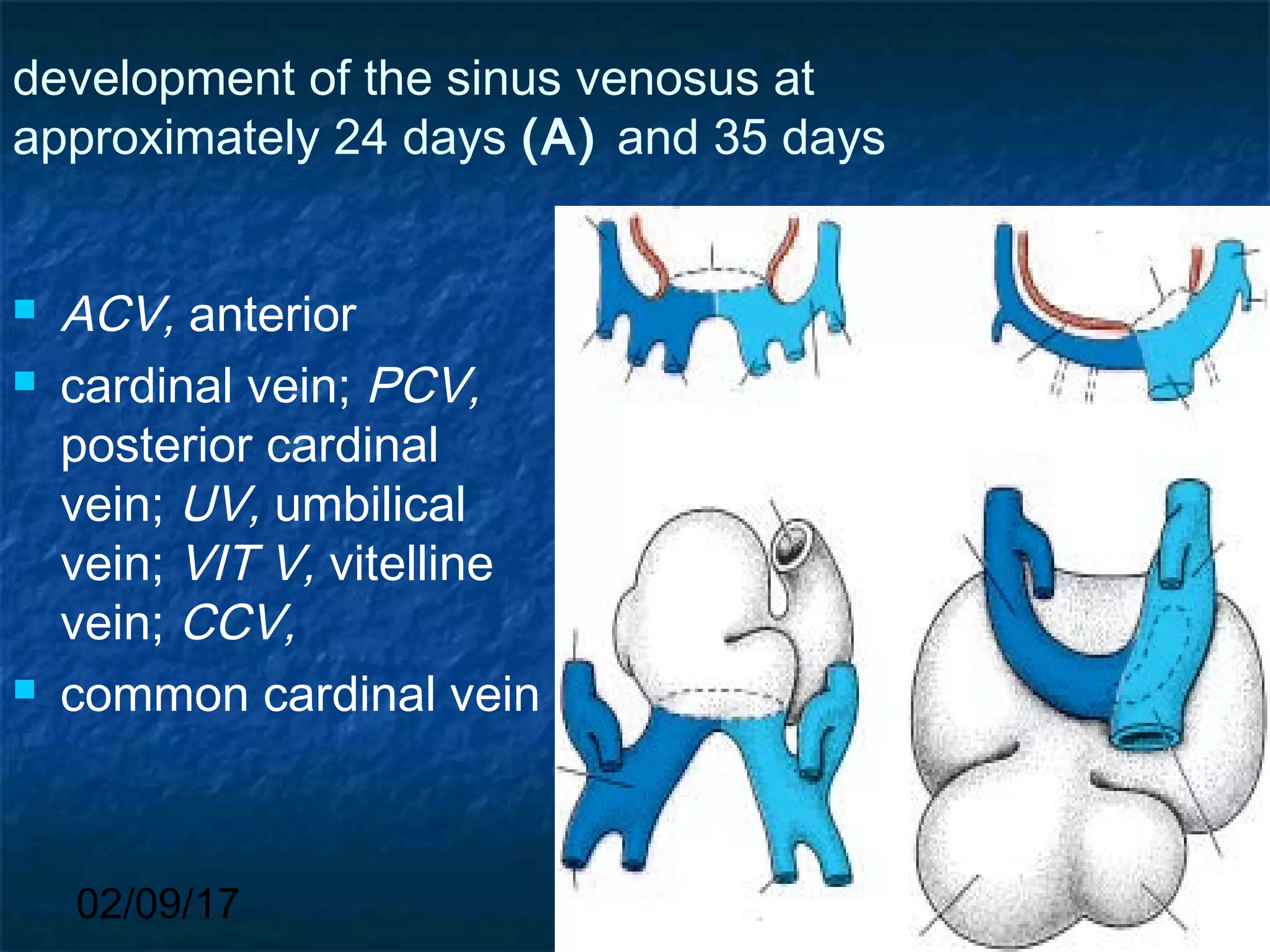
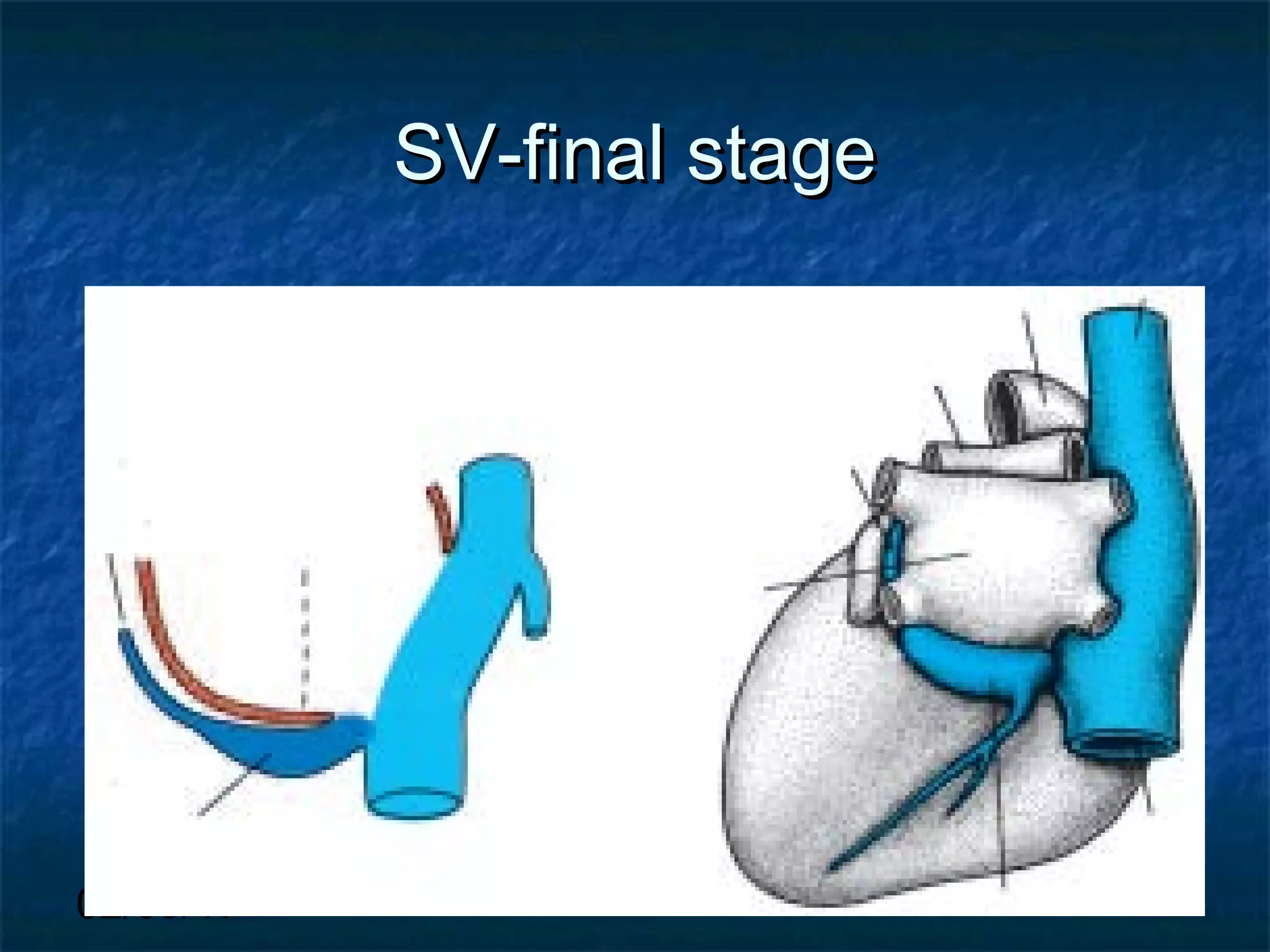
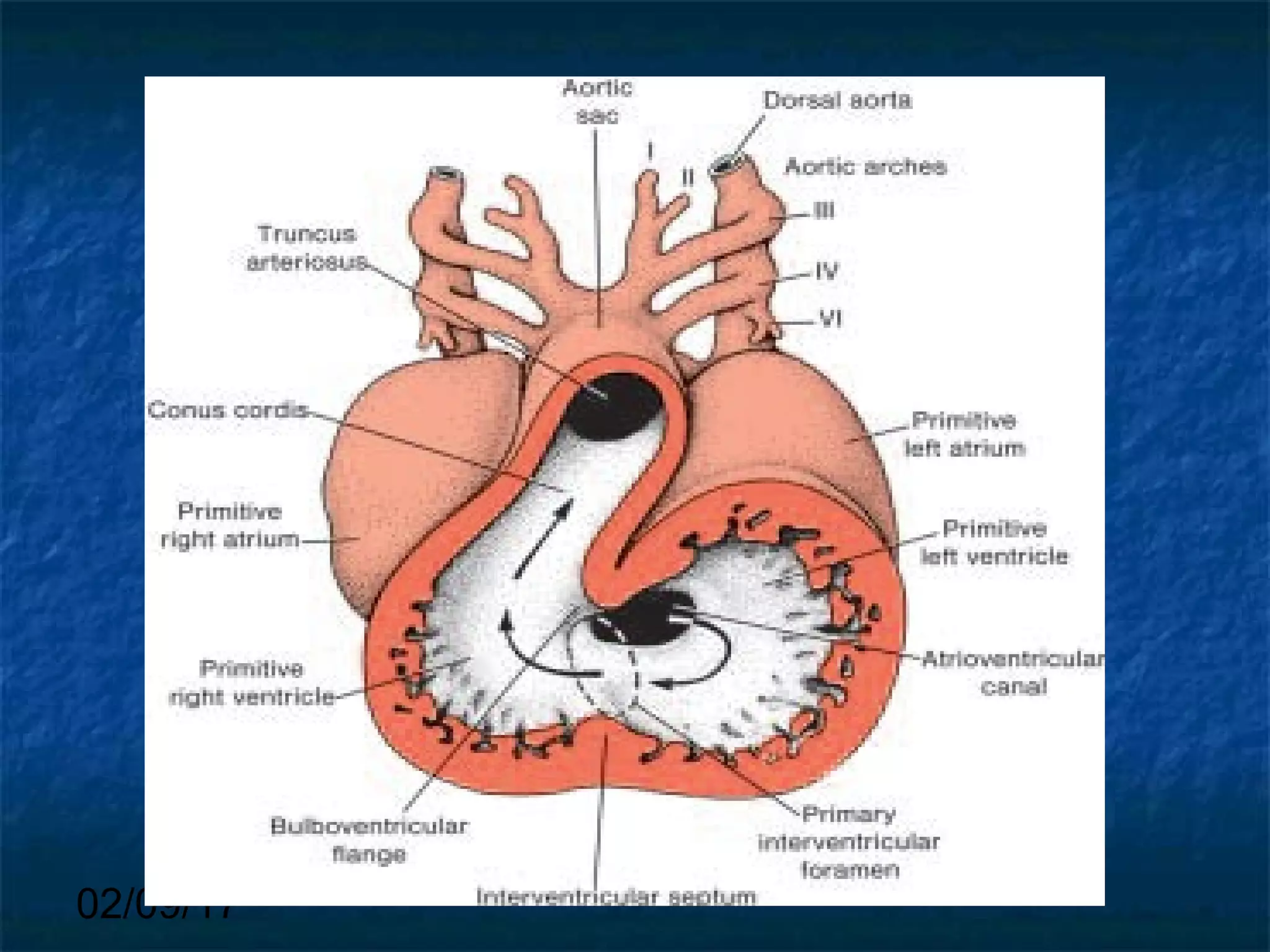
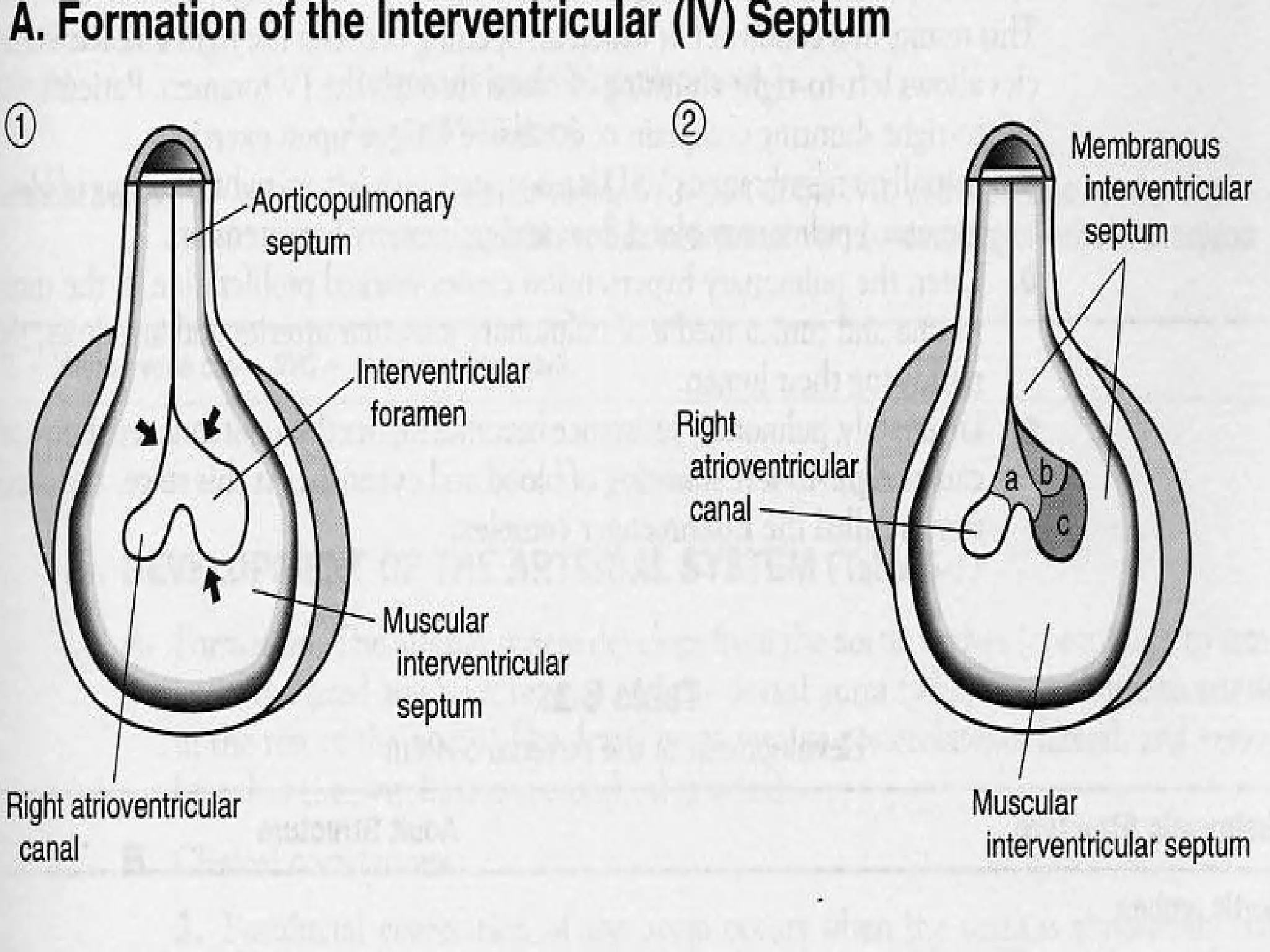
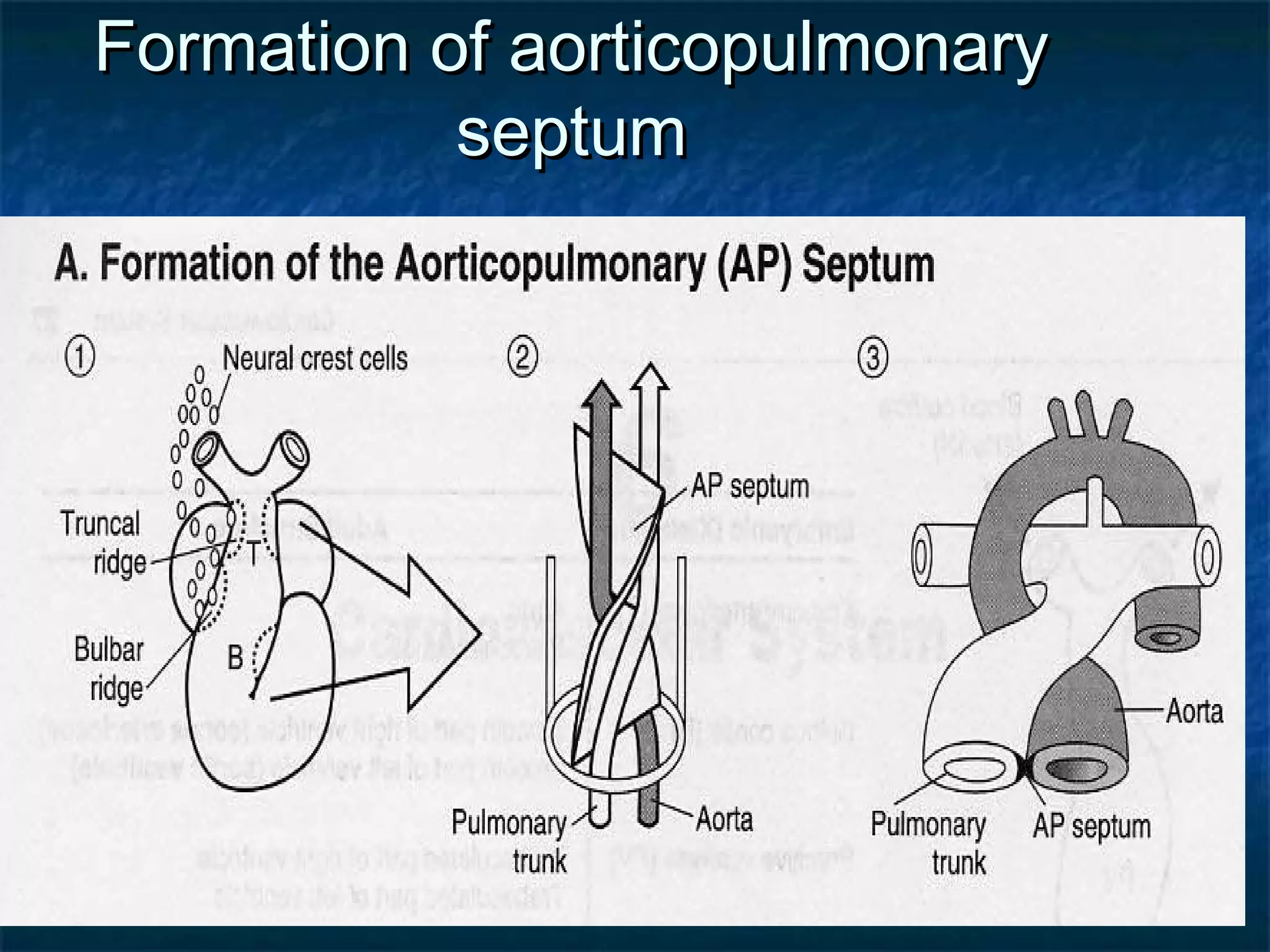
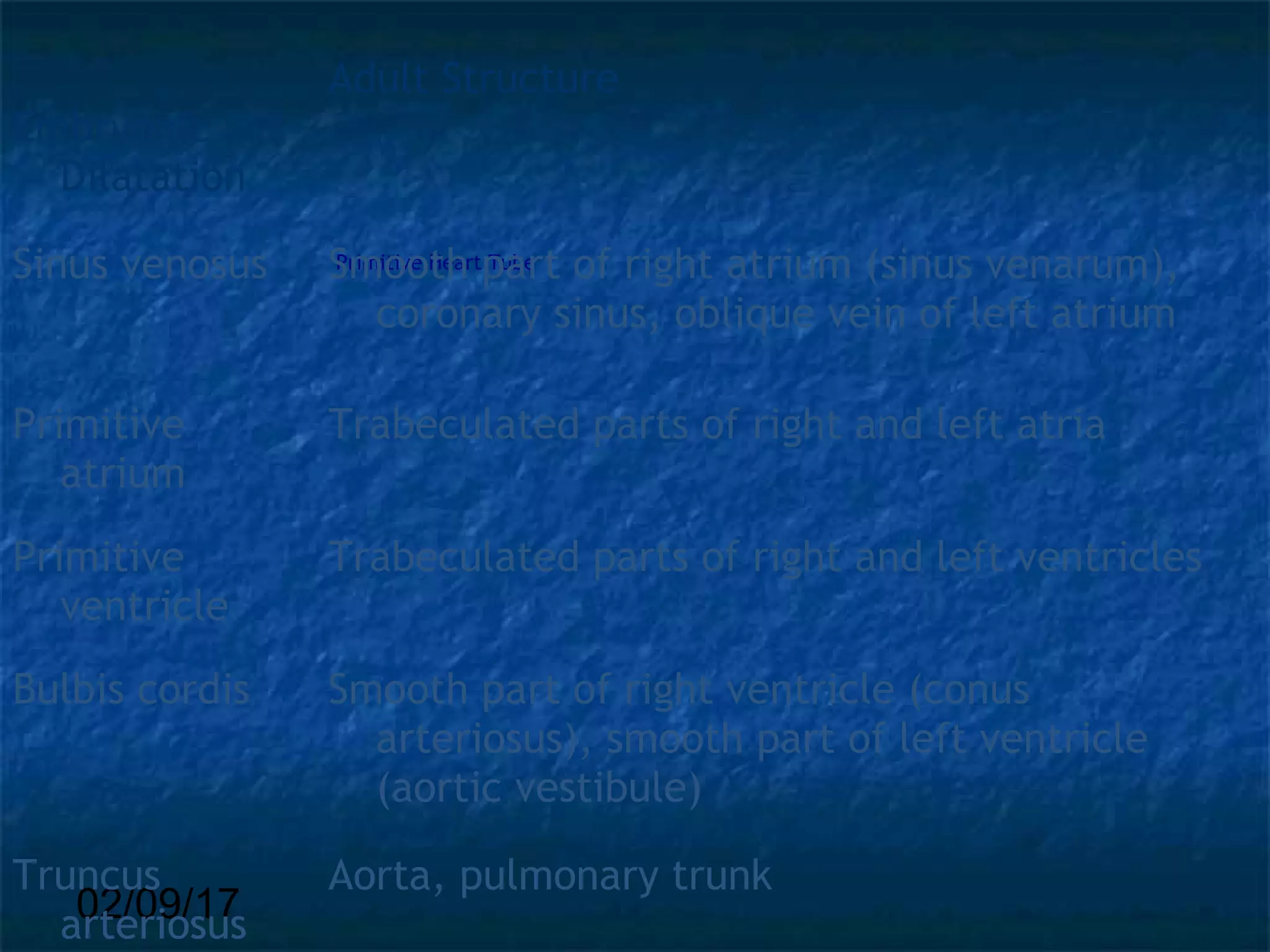
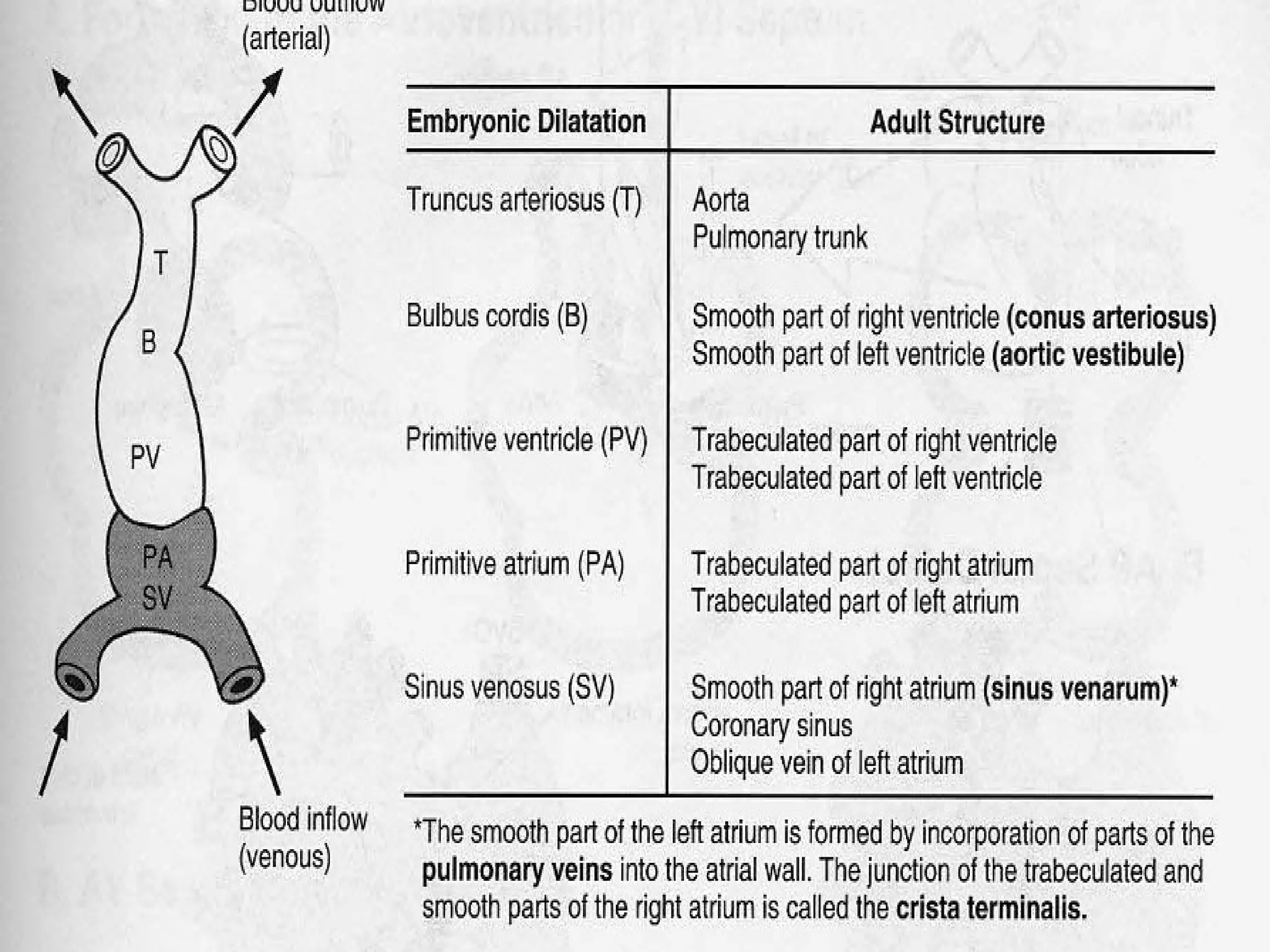
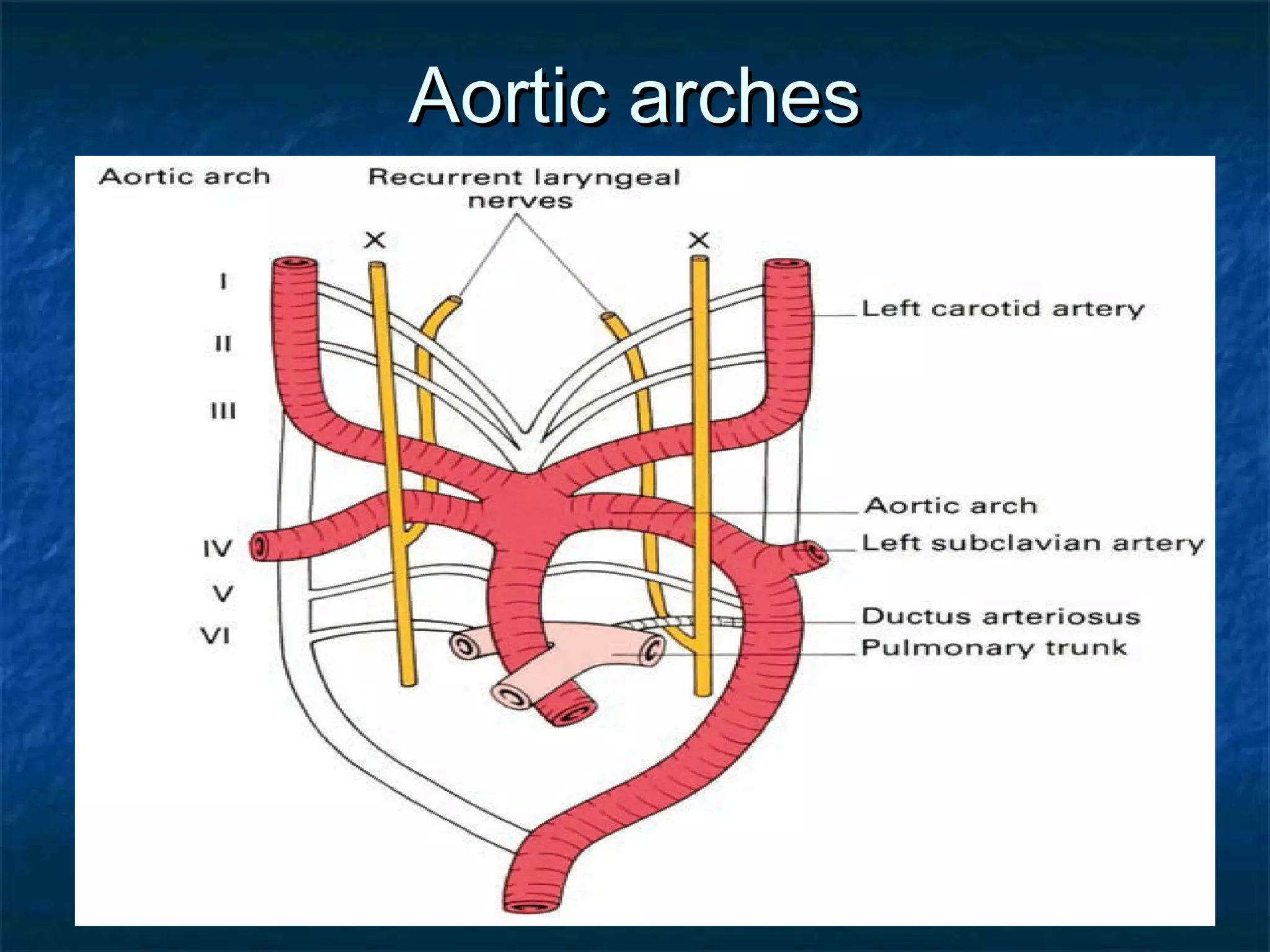
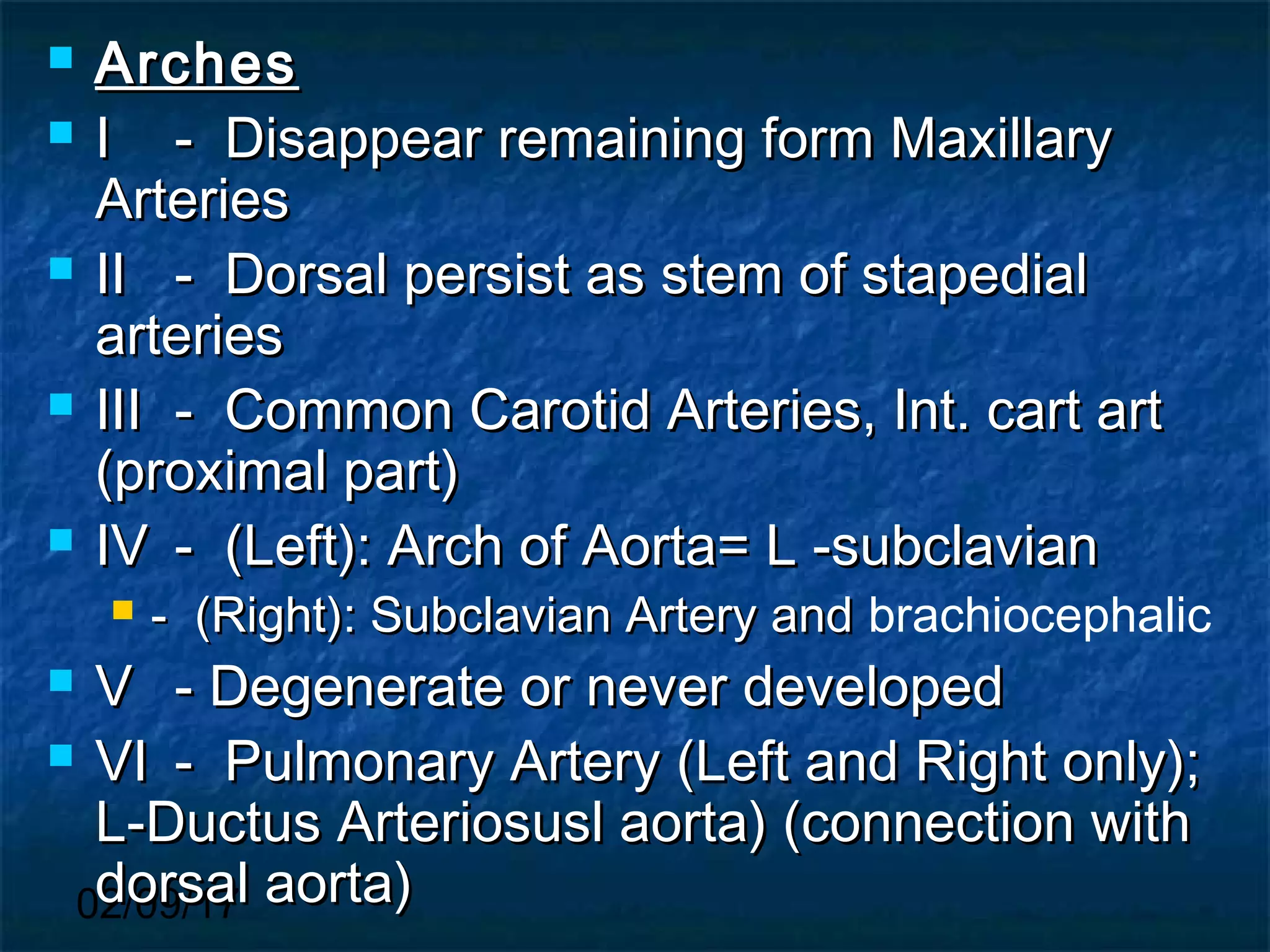
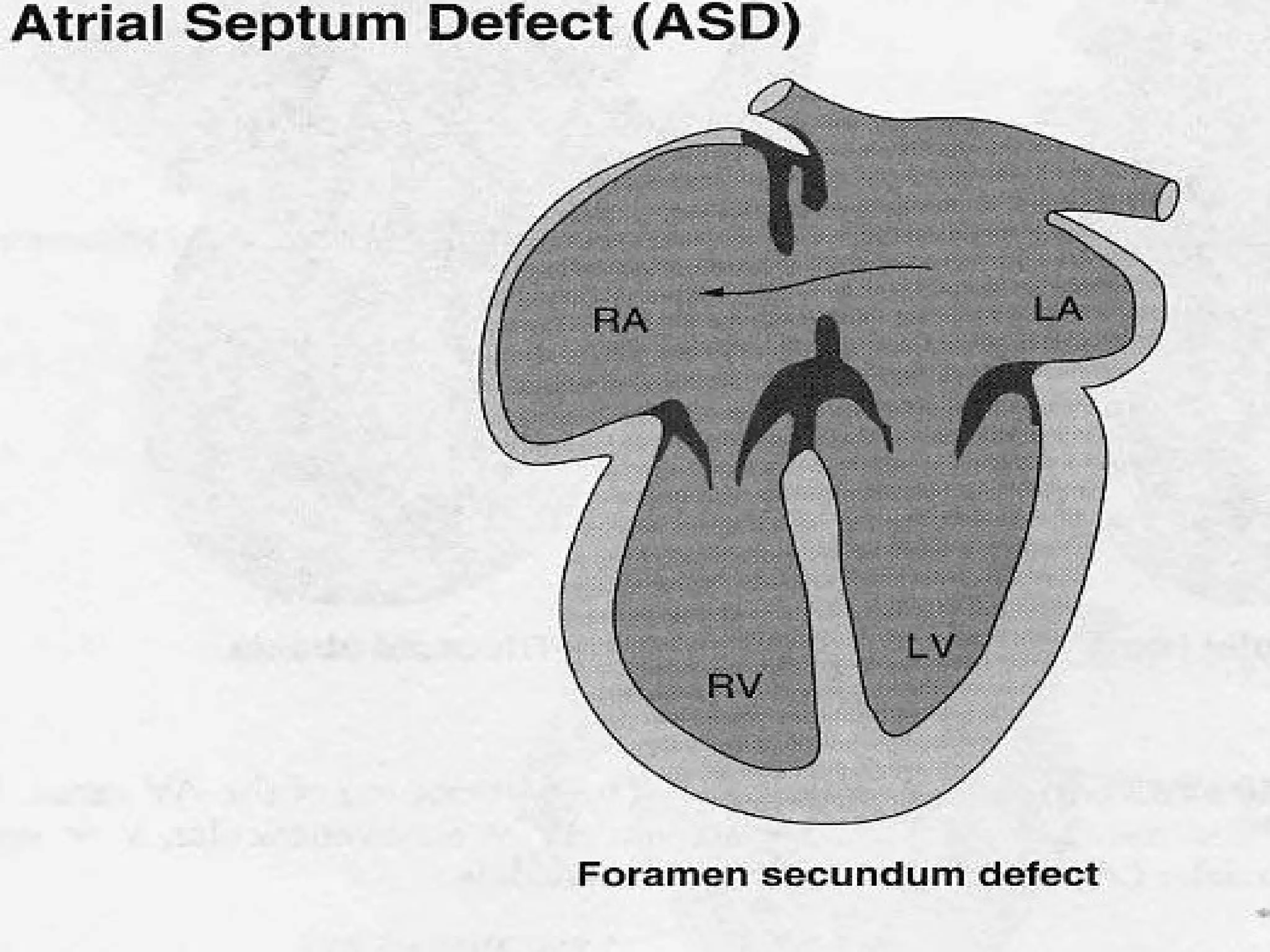
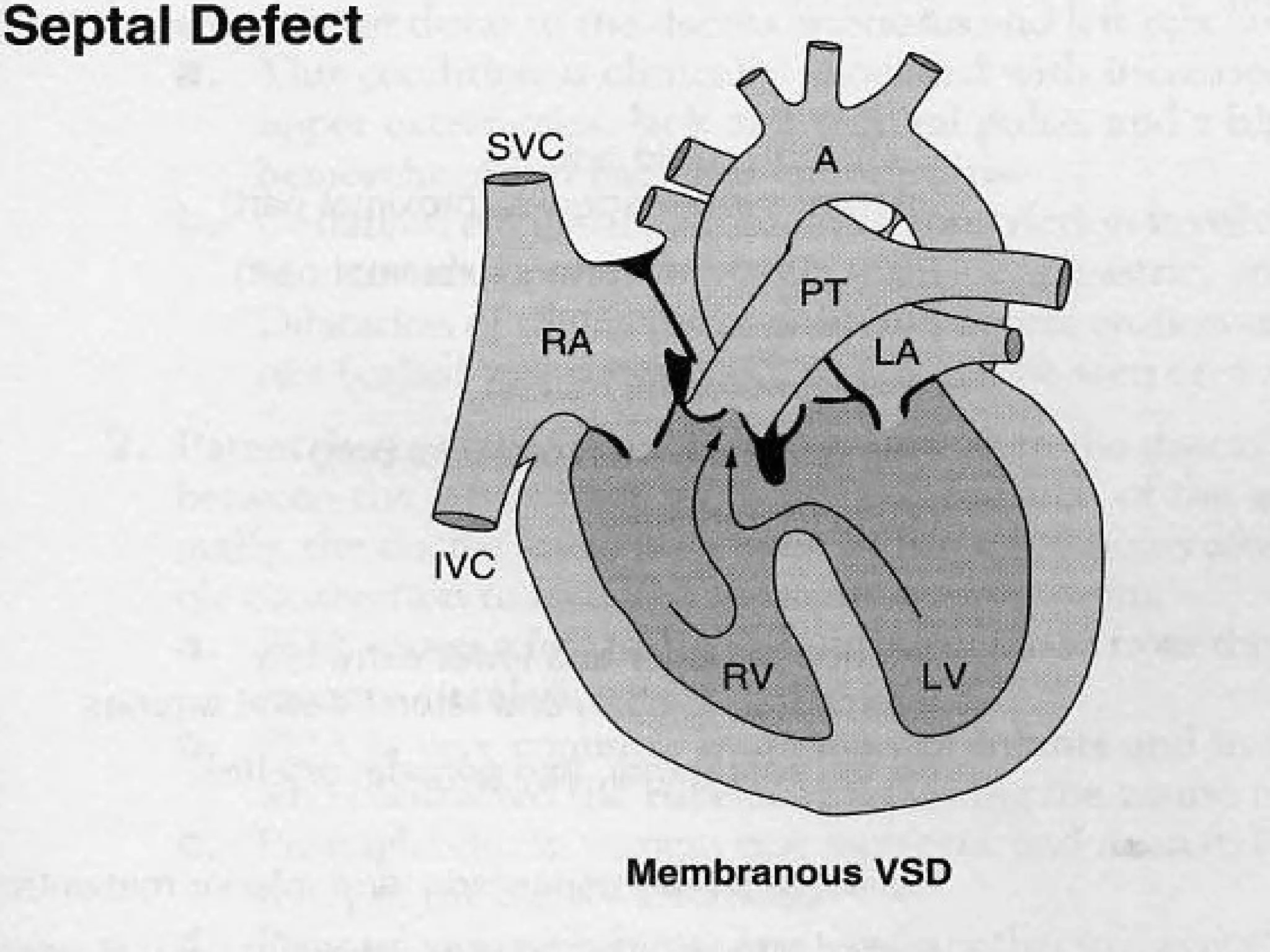
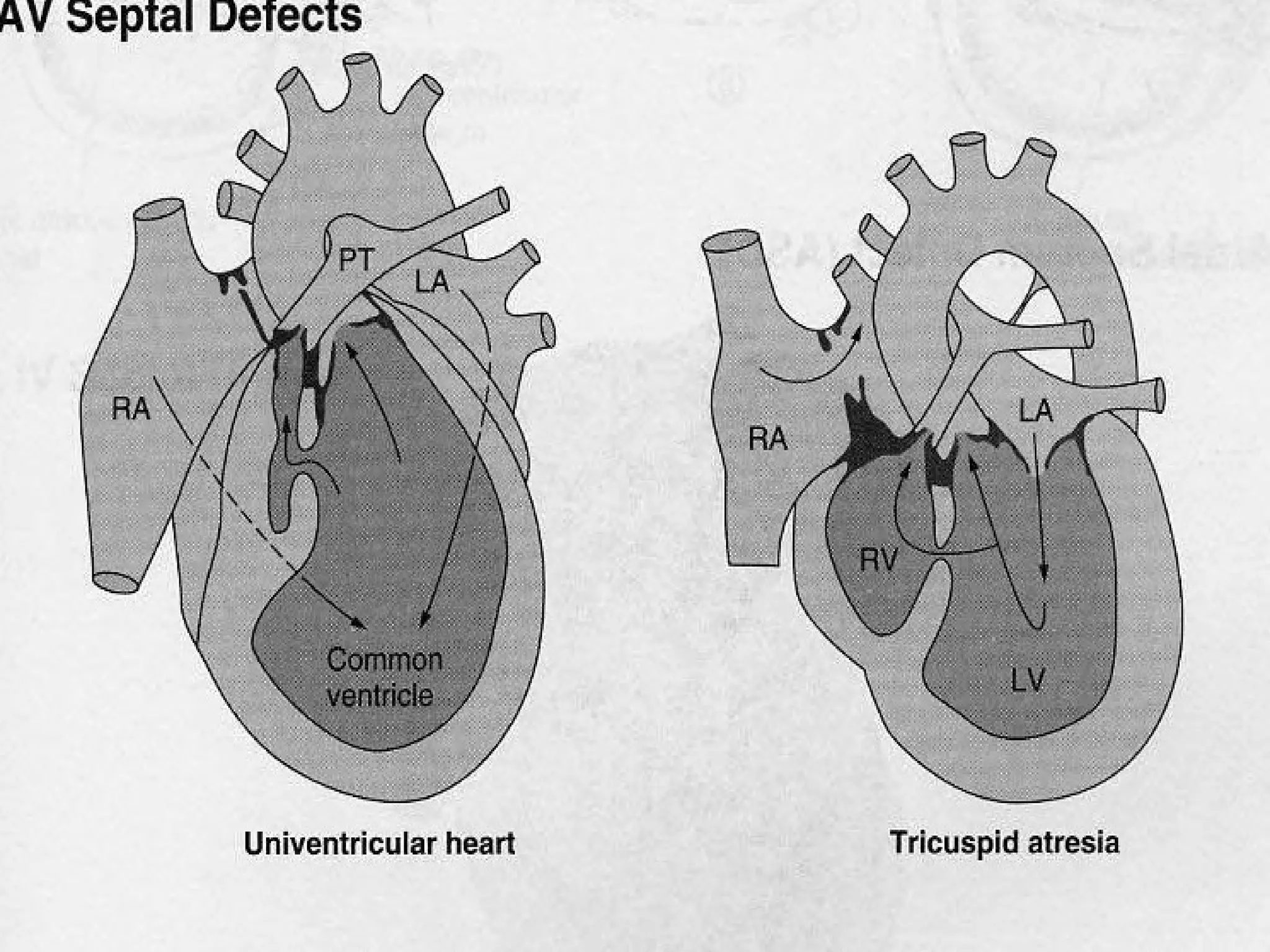
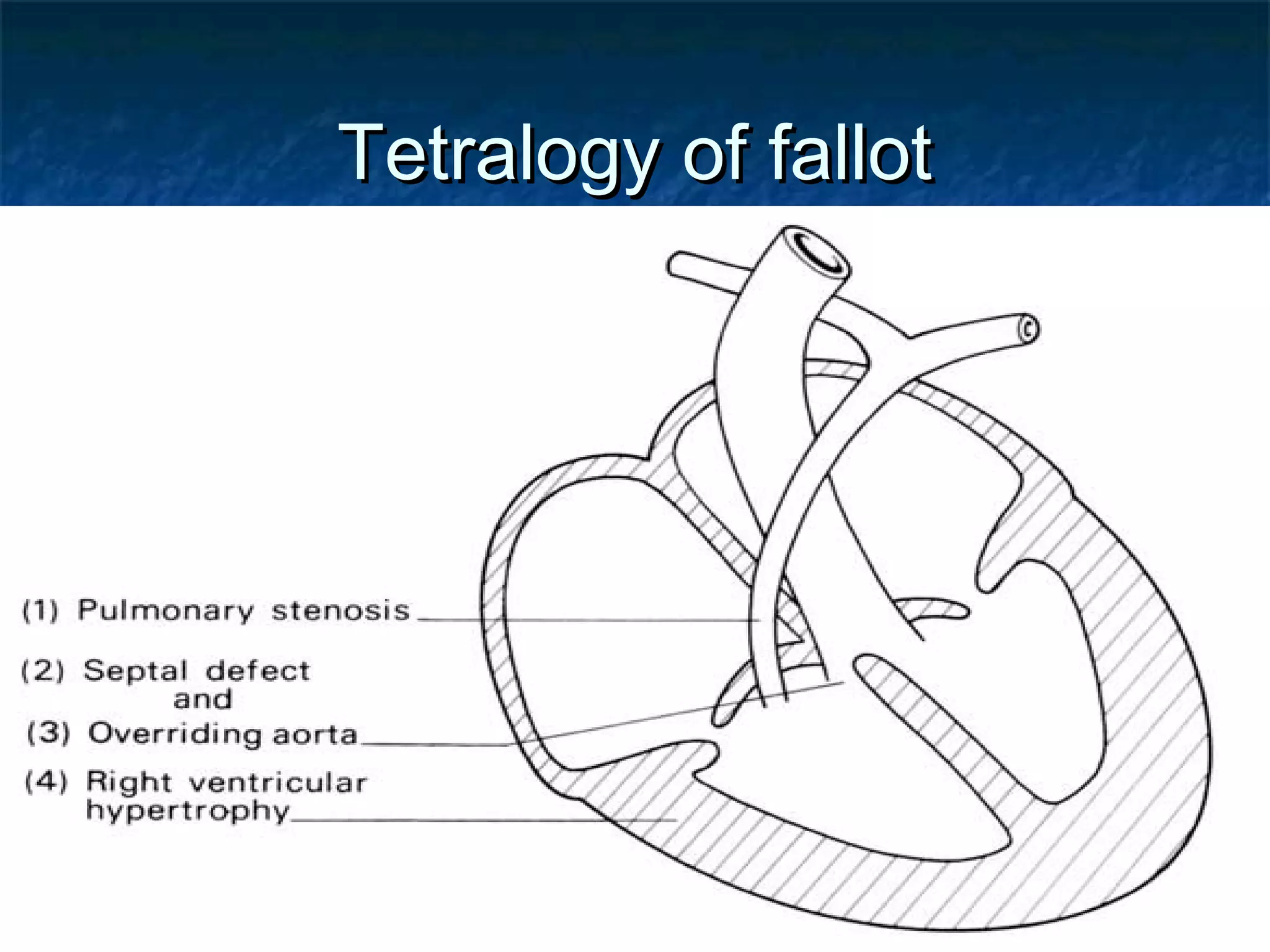
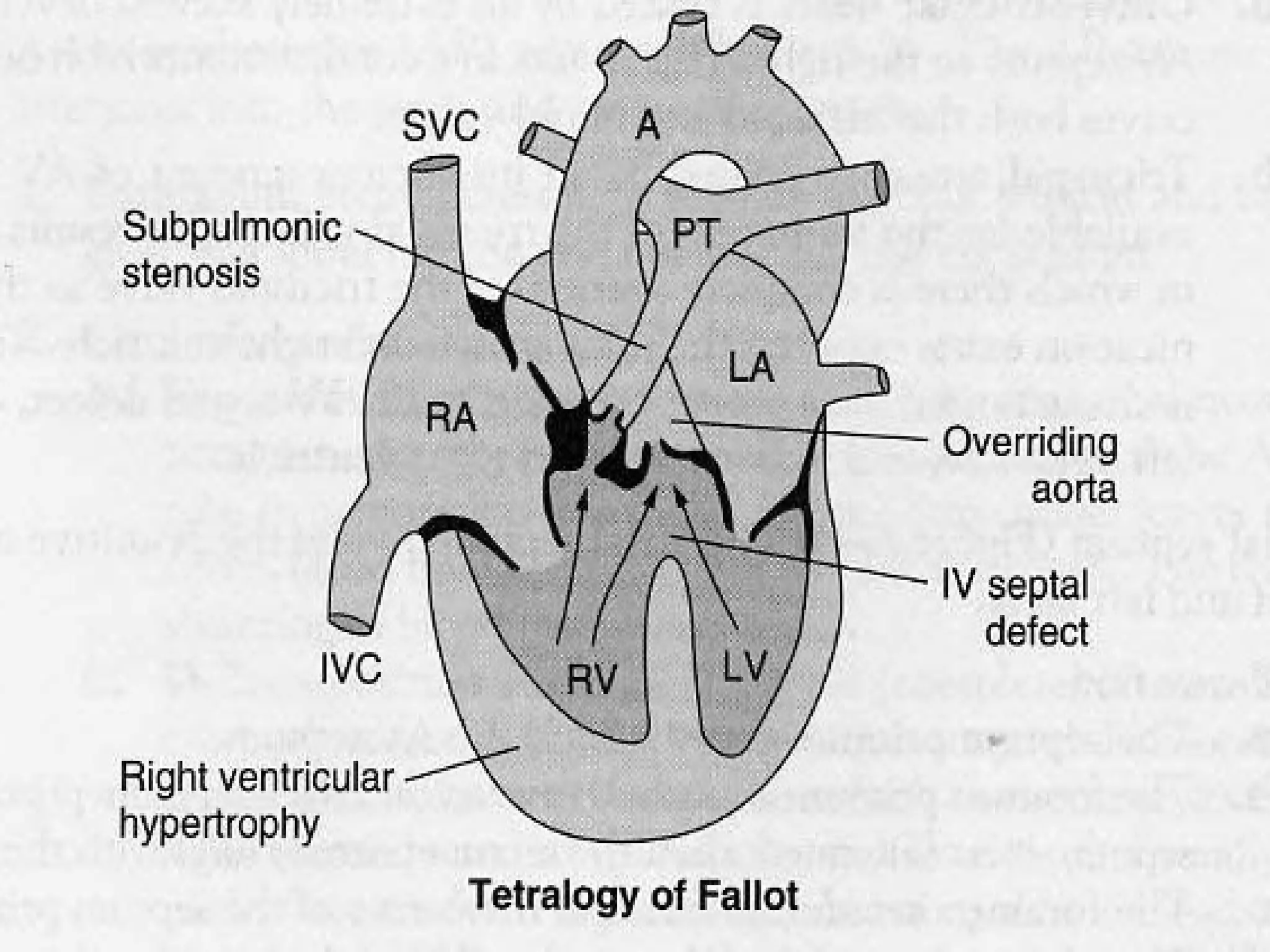
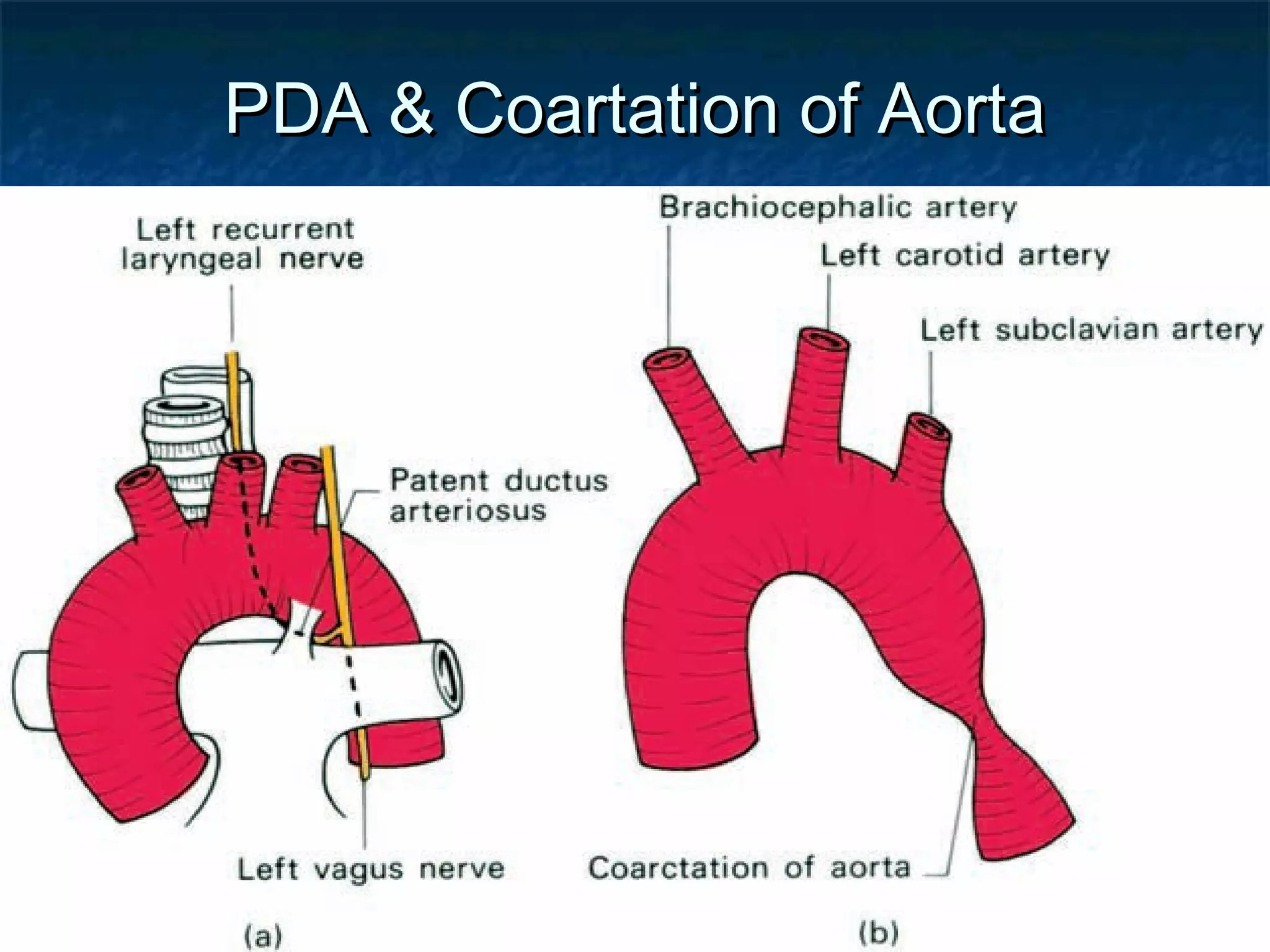
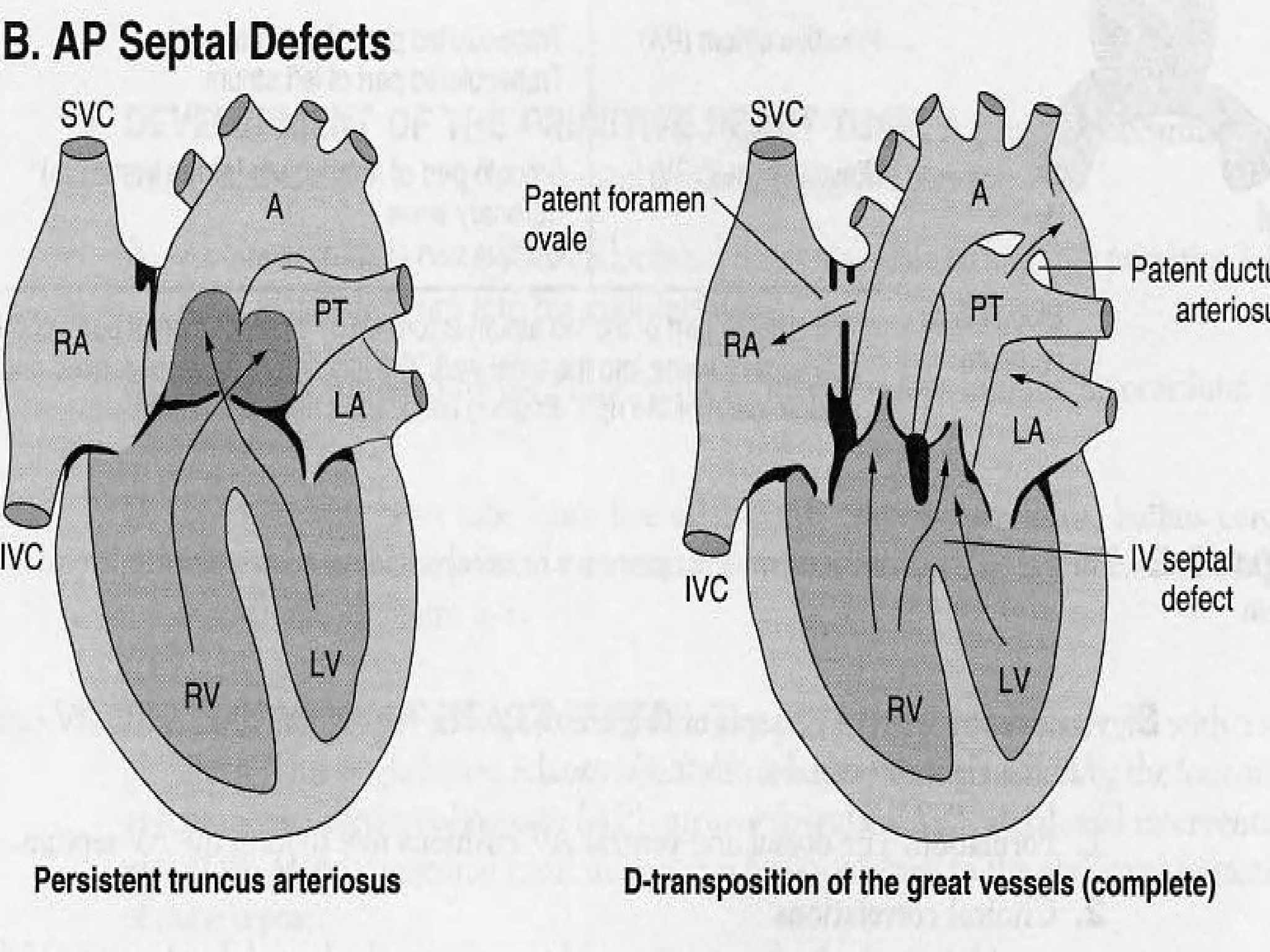
3. Partitioning of the heart chambers by growth of septa that divide the atria and ventricles, forming the four-chambered heart, and division of the truncus arteriosus into the aorta and pulmonary trunk.















































![Embryology [heart.].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/embryologyheart-230508191331-cc41d237-thumbnail.jpg?width=640&height=640&fit=bounds)






































