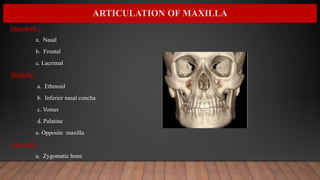
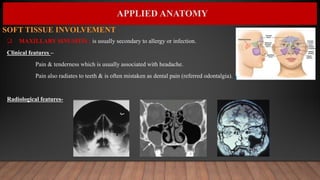
The document provides information about a seminar on the maxilla presented by Dr. Mrinalini Singh. It includes details on the development, anatomy, articulations, ossification, muscles, blood supply, innervation, and age changes of the maxilla bone. The maxilla forms the upper jaw and parts of the face, nose, mouth, orbit, and paranasal sinuses. It articulates with several bones including the nasal, frontal, lacrimal, ethmoid, vomer, palatine, opposite maxilla, and zygomatic. The maxilla contains the maxillary sinus and has processes including the frontal, zygomatic, alveolar, and palatine processes. Applied anatomy discusses























































![Growth & development of maxilla & mandible.ppt [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/growthdevelopmentofmaxillamandible-180610064645-thumbnail.jpg?width=640&height=640&fit=bounds)
![PRE-NATAL GRnnnmnnnnmmOWTH seminar[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pre-natalgrowthseminar1-250427093235-de04befc-thumbnail.jpg?width=640&height=640&fit=bounds)
























