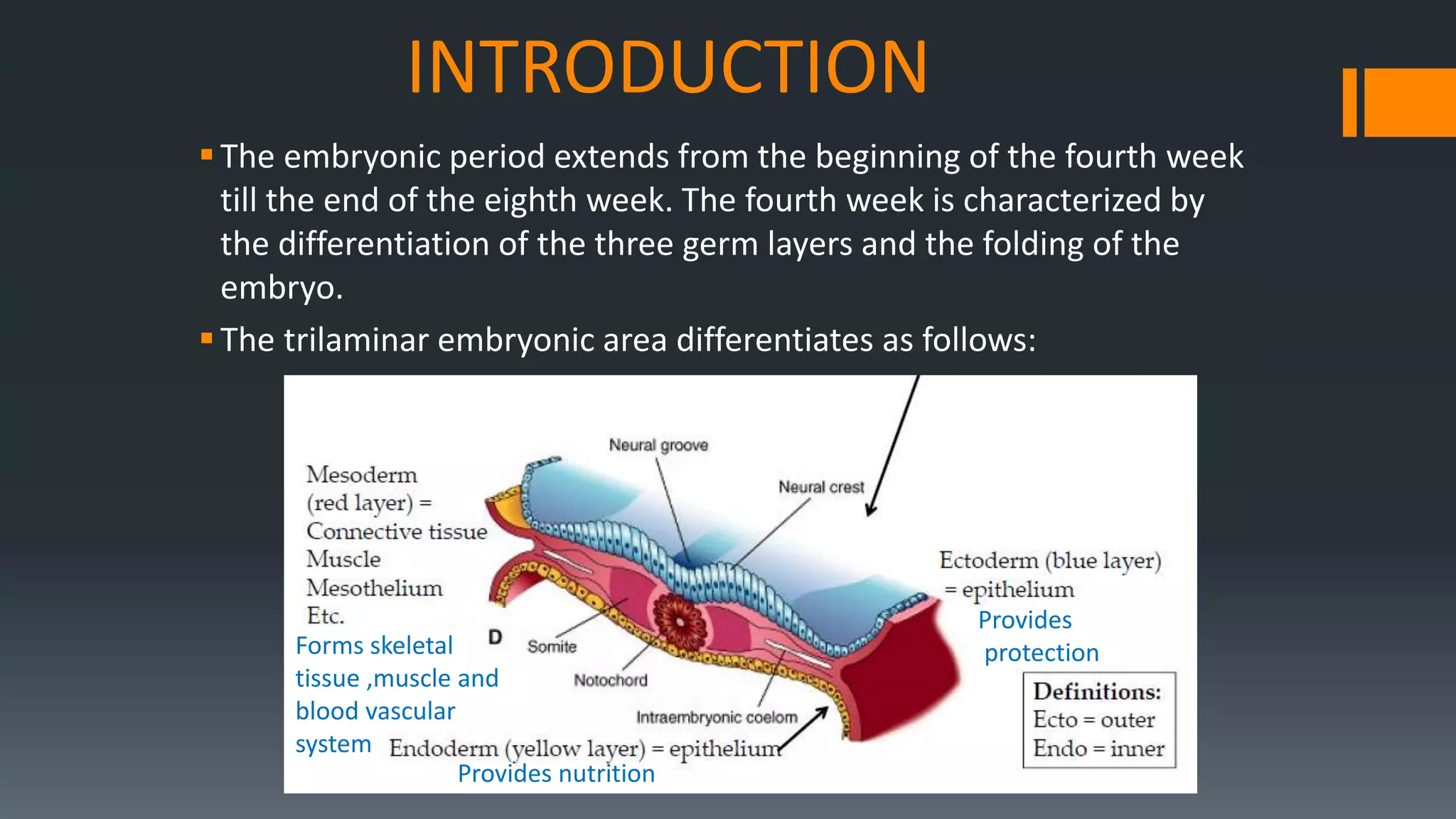
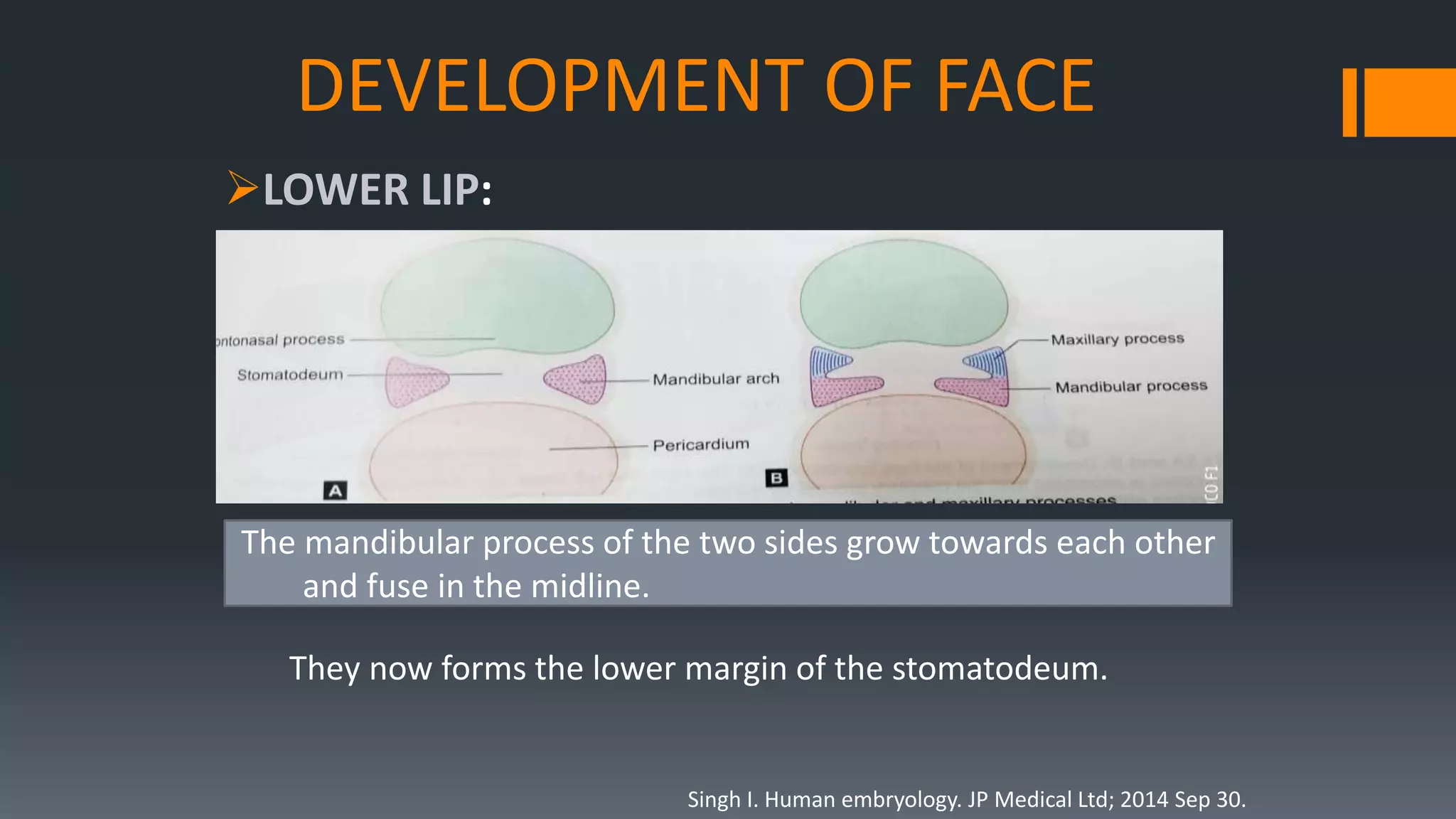
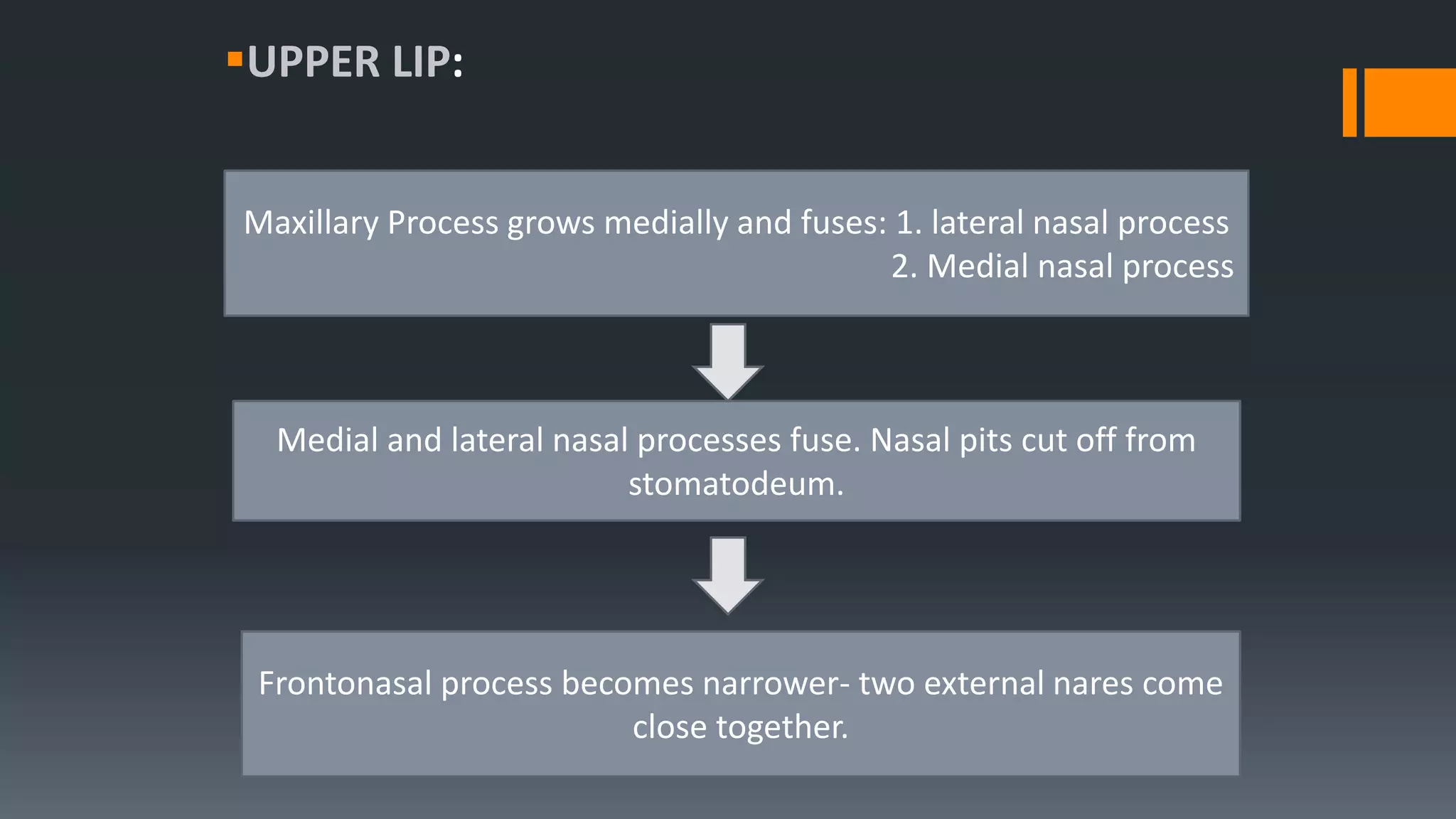
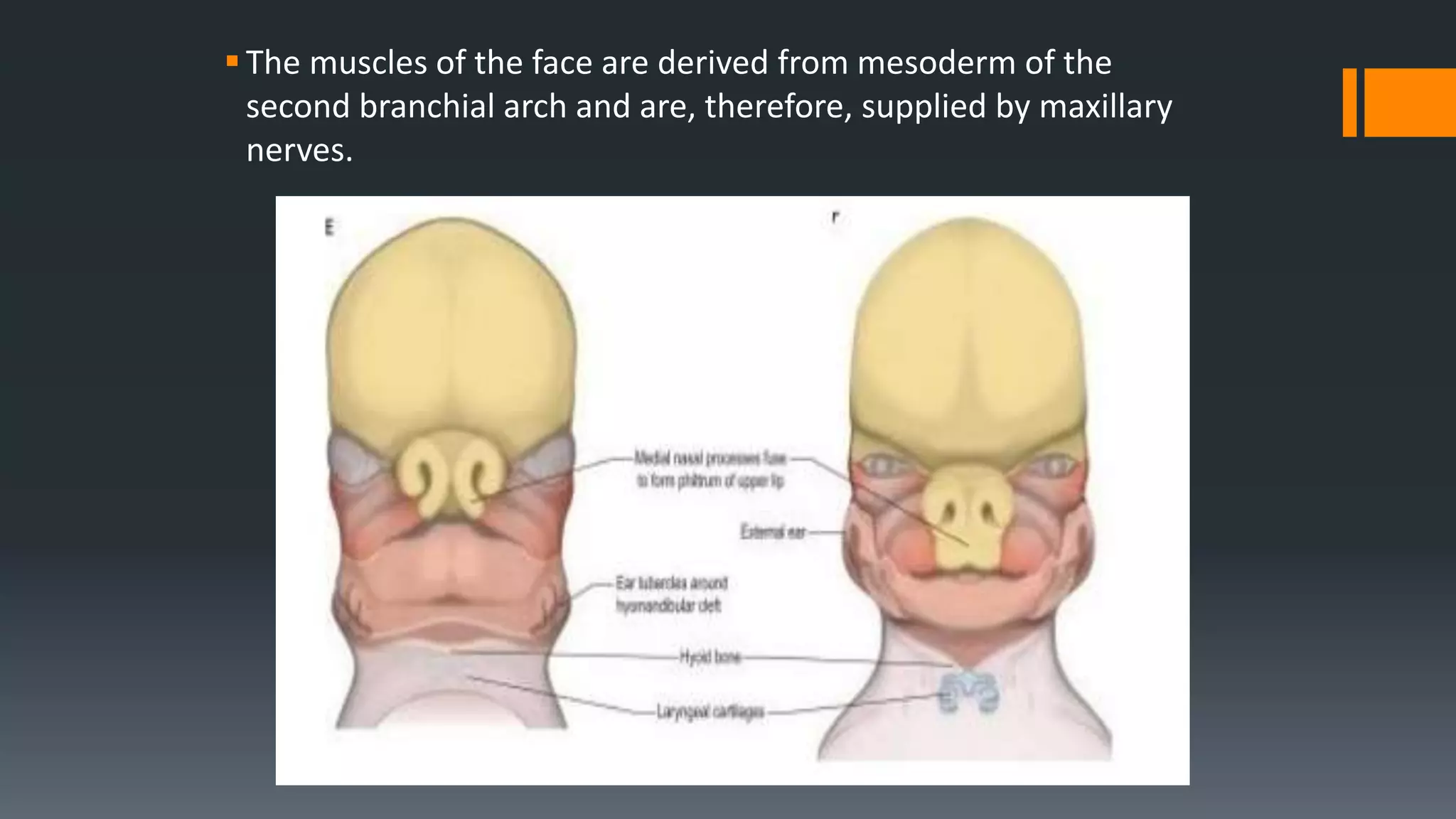
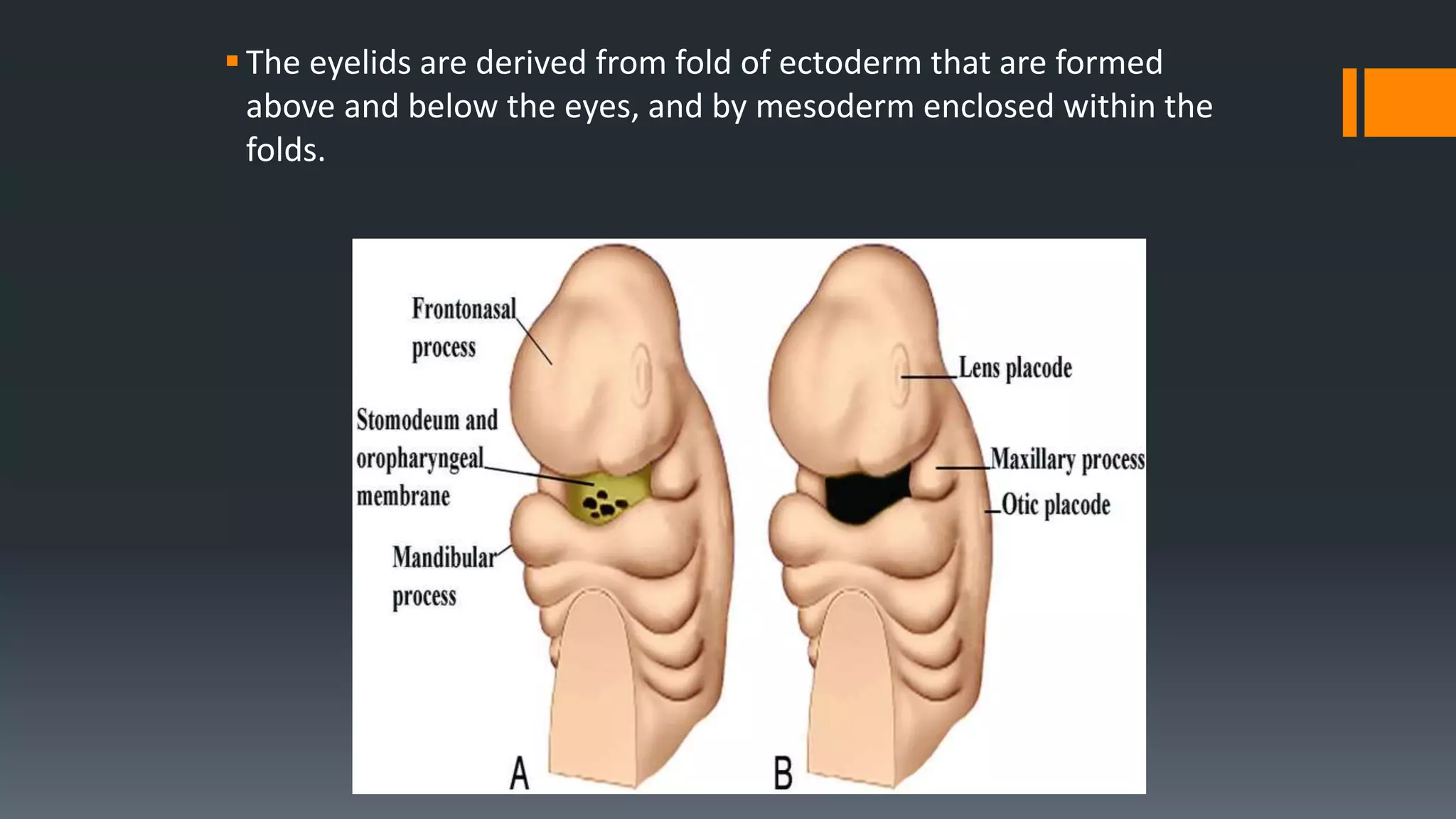
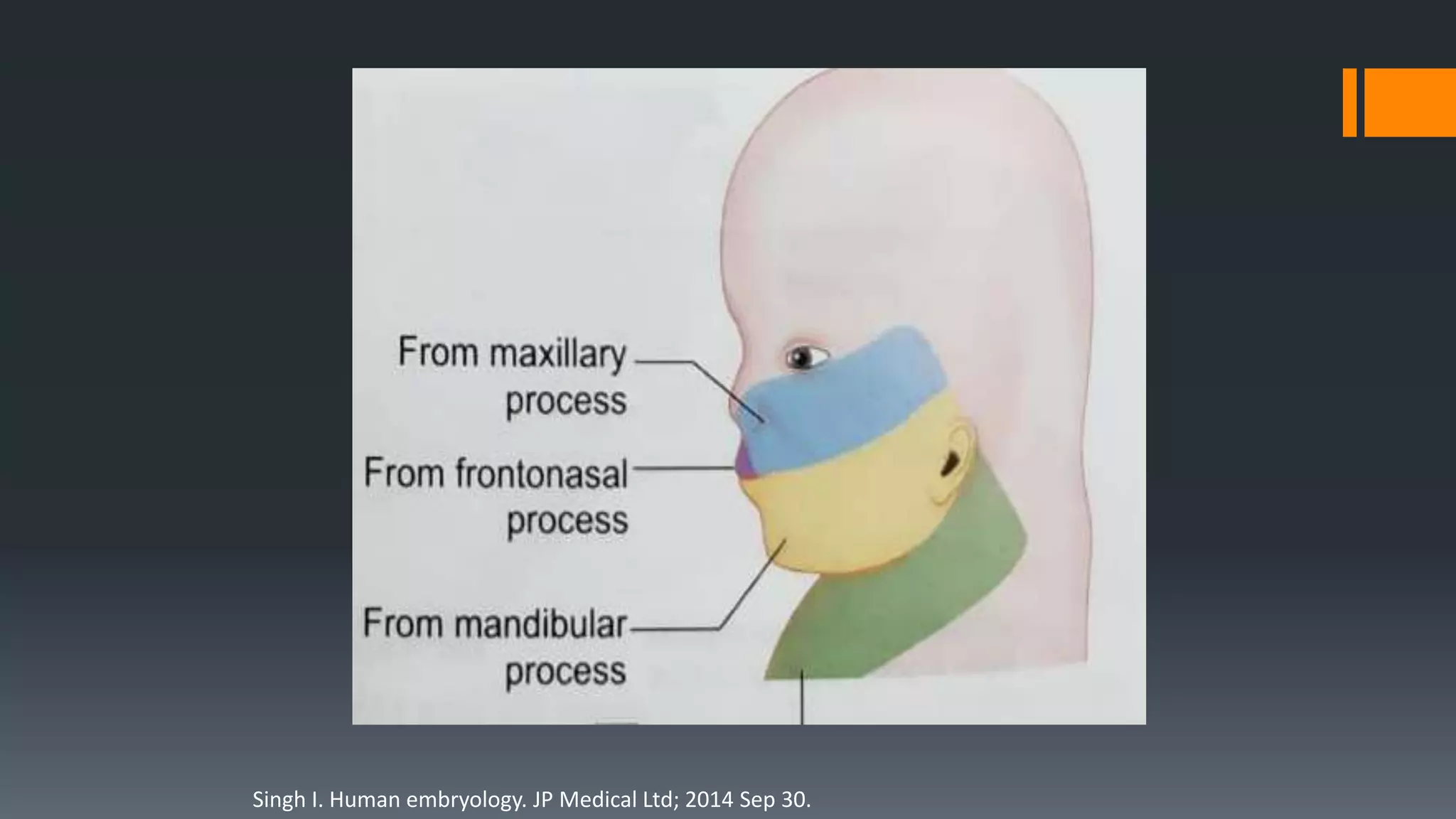
The document discusses the development of the face and palate in humans. It describes how the face develops from structures around the stomatodeum, including the frontonasal process and first pharyngeal arch. The lips, nose, cheeks, eyes, and ears develop through the growth and fusion of these structures between 4-8 weeks. The palate develops from the primary and secondary palate, which grow towards each other and fuse between 6-12 weeks. Possible developmental anomalies that can occur if this process is disrupted include cleft lip, cleft palate, and abnormalities in the size and position of facial features.





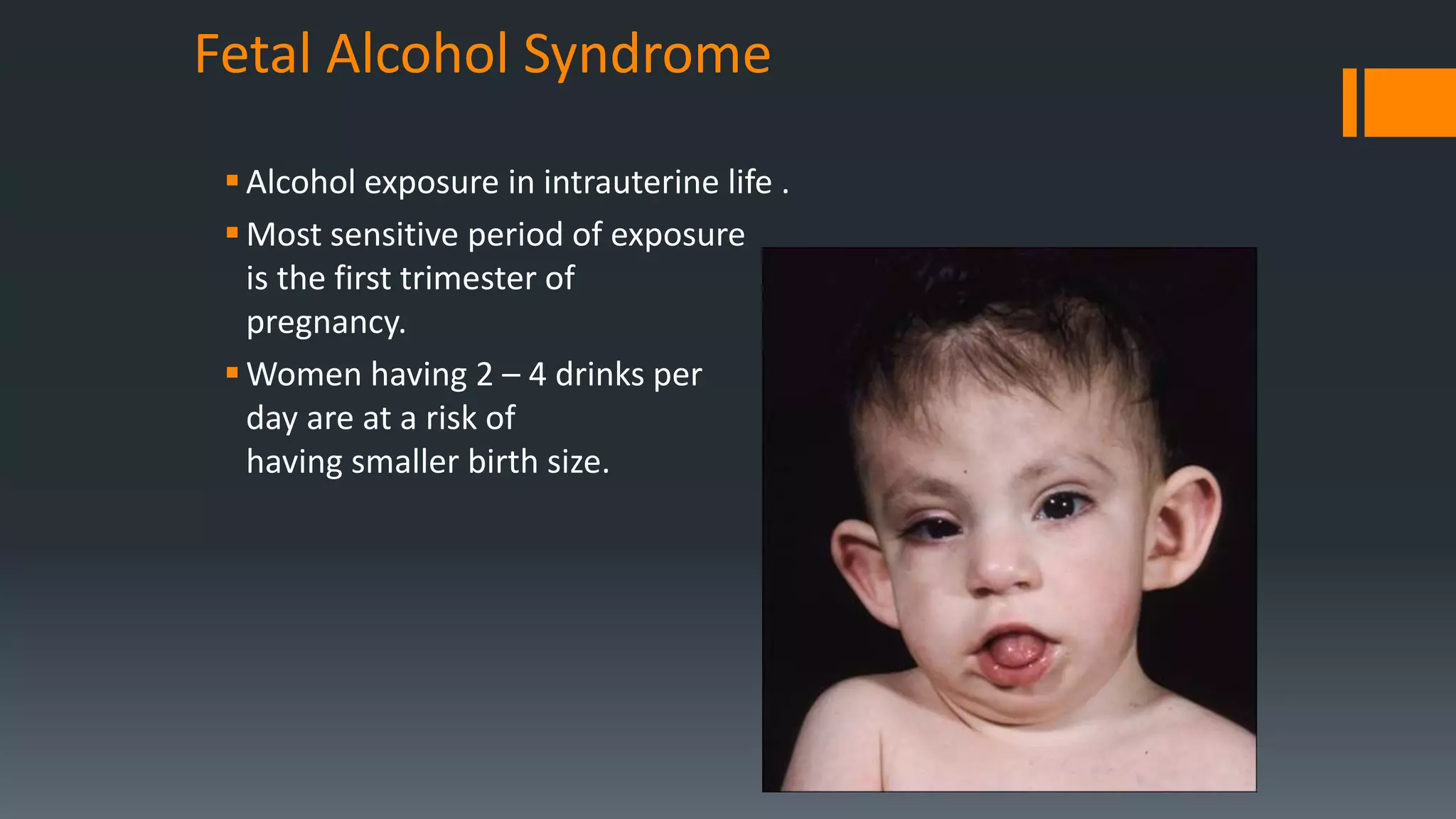
![Clinical features:
1. Short palpebral fissures,
2. Thin vermillion border,
3. Smooth philtrum,
4. In-utero and postnatal growth retardation,
5. Microcephaly,
6. Maxillary hypoplasia,
7. Micrognathia,
8. Decreased interpupillary distance,
9. Structural defects may also occur in the cardiovascular, renal,
musculoskeletal, ocular, and auditory systems.
Vorgias D, Bernstein B. Fetal Alcohol Syndrome. InStatPearls [Internet] 2017 Nov 19.
StatPearls Publishing.](https://image.slidesharecdn.com/developmentoffaceandpalate-201011152944/75/Development-of-face-and-palate-65-2048.jpg)
![REFERENCES
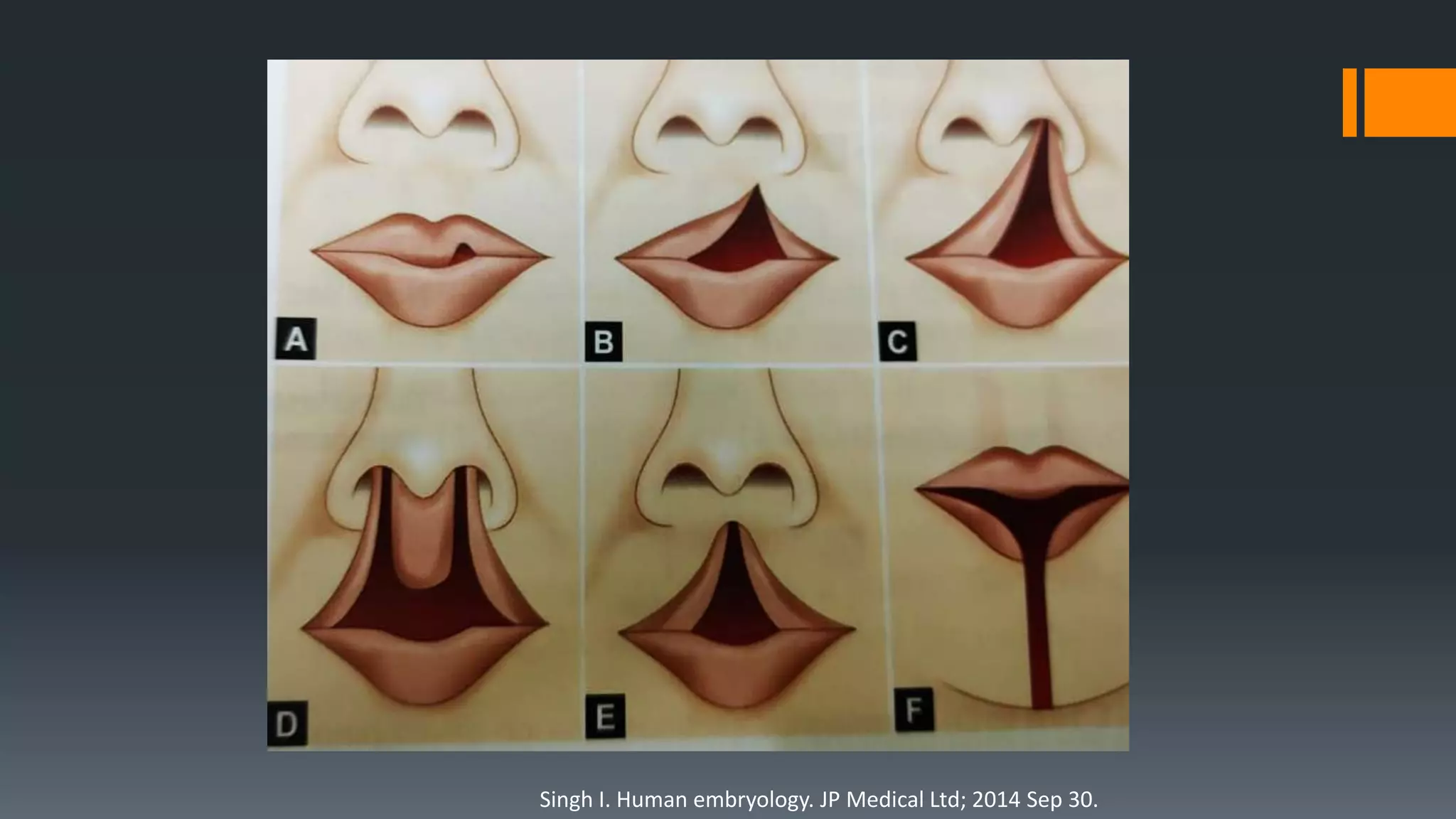
1. Singh I. Human embryology. JP Medical Ltd; 2014 Sep 30.
2. Sadler TW. Langman's medical embryology. Lippincott Williams & Wilkins;
2011 Dec 15.
3. Beumer J, Curtis TA, Firtell DN. Maxillofacial rehabilitation. St. Louis: Mosby.
1979:90-169.
4. Ibrahim A, Ajike S. Congenital symmetrical lower lip pits: Van der Woude
syndrome. Oman medical journal. 2015 Jan;30(1):e081.
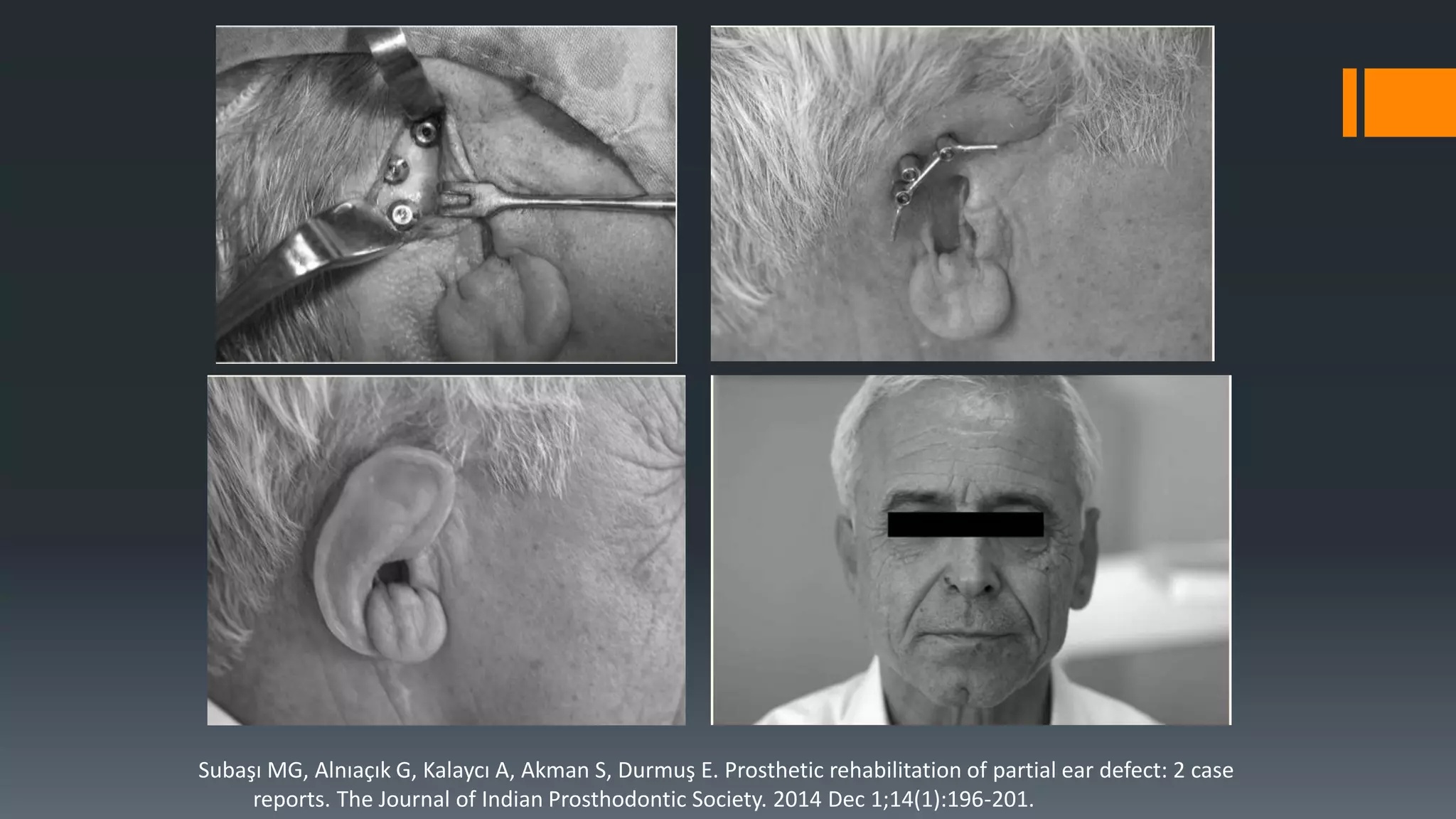
5. Subaşı MG, Alnıaçık G, Kalaycı A, Akman S, Durmuş E. Prosthetic rehabilitation
of partial ear defect: 2 case reports. The Journal of Indian Prosthodontic
Society. 2014 Dec 1;14(1):196-201.
6. Ranjith Kumar P. et al.: Prosthetic Consideration in Management of Cleft Lip
and Palate Patients
7. Vorgias D, Bernstein B. Fetal Alcohol Syndrome. InStatPearls [Internet] 2017
Nov 19. StatPearls Publishing.
8. Parameswaran A, Ramanathan M. Hemifacial microsomia. Journal of Indian
Orthodontic Society. 2018 Jul 1;52(3):155-.](https://image.slidesharecdn.com/developmentoffaceandpalate-201011152944/75/Development-of-face-and-palate-67-2048.jpg)














































































