Downloaded 259 times
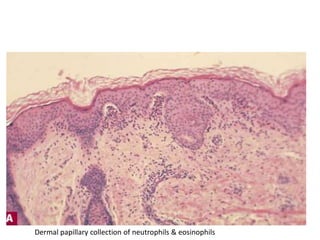
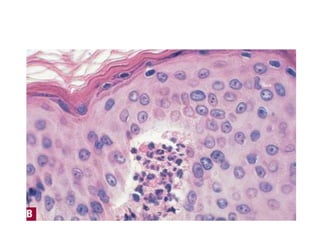
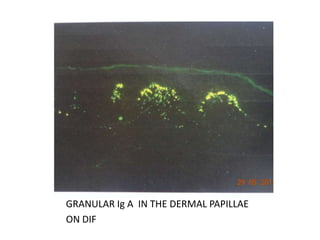
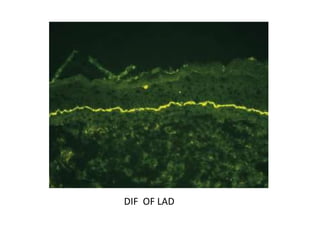
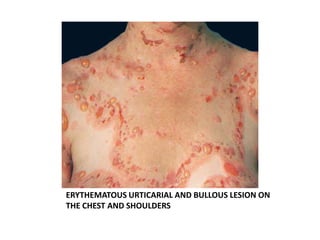
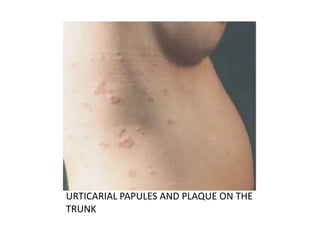


Dermatitis herpetiformis is a chronic blistering skin disease characterized by intensely pruritic grouped vesicles arising on an erythematous base. It is associated with gluten sensitivity and asymptomatic enteropathy. Linear IgA disease is a chronic autoimmune subepidermal blistering disease characterized by linear deposition of IgA along the dermoepidermal junction. It can present in both children and adults, with childhood presentations typically featuring large tense bullae on the genitalia and buttocks arranged in clusters. Adult presentations are more variable with flexural involvement and features resembling bullous pemphigoid in some cases. Both diseases involve neutrophilic infiltration and IgA deposition but have different pathogenic mechanisms and associations.



































































