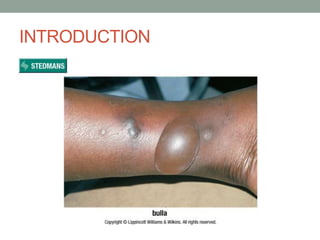
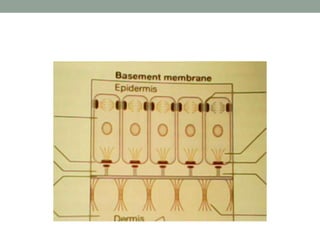
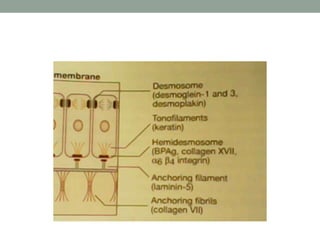
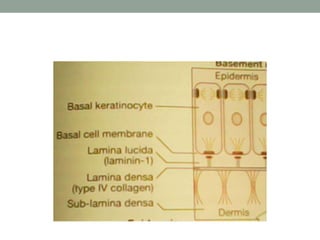
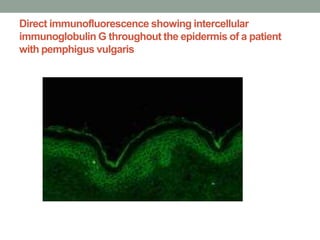
This document provides information on bullous skin disorders. It begins by defining a bulla or blister. Bullous skin disorders are characterized by the presence of blisters or erosions on the skin and mucous membranes. These disorders are usually due to autoimmune diseases or inherited abnormalities of structural proteins found in the epidermis and basement membrane. Bullous skin disorders can be divided into immunobullous or mechanobullous categories. Several specific immunobullous disorders are described in detail including their pathogenesis, clinical features, diagnosis, and treatment.
![Pemphigus vegetans
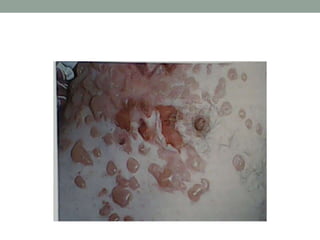
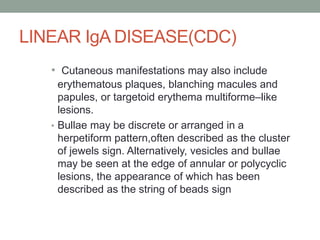
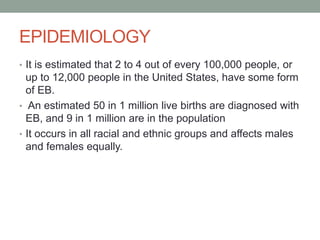
• Pemphigus vegetans is a variant of p.
vulgaris, Presents with a large moist
verrucous [wart-like] vegetating plaques
with pustules.
• by proliferative and verrucous lesions on
the erosions
• a rare form that do not present with blisters
• Distribution includes groin, axillae, and
flexural surfaces.](https://image.slidesharecdn.com/bullousskindisorders-231212212736-aa380dc2/85/BULLOUS-SKIN-DISORDERS-ppt-26-320.jpg)












































![[Chronic Multiple ulcers] O.Medicine lab](https://cdn.slidesharecdn.com/ss_thumbnails/o-250128123323-29e53ff5-thumbnail.jpg?width=640&height=640&fit=bounds)




































![[DSC Europe 25] Josip Saban - Career building for data professionals.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/zroflcttkm1vmli0txea-josip-saban-career-building-for-data-professionals-260123083019-587cdb8c-thumbnail.jpg?width=640&height=640&fit=bounds)









