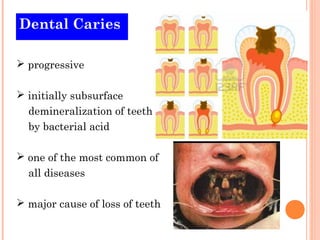
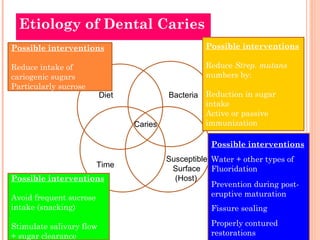
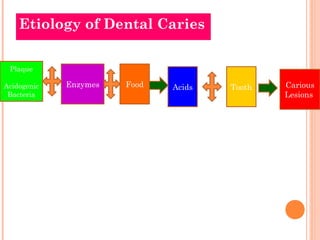
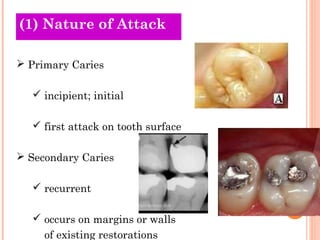
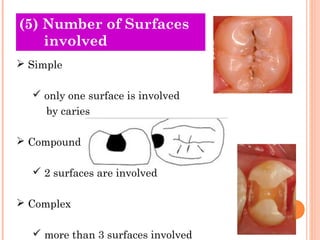
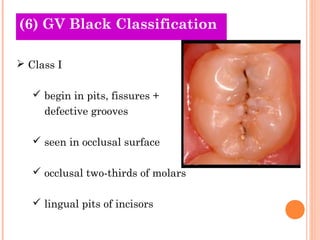
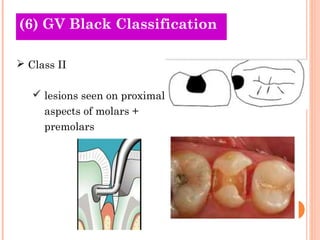
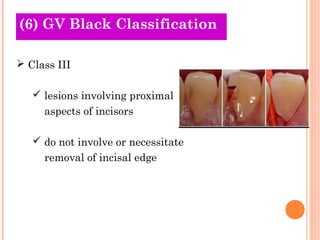
Dental caries is a progressive, subsurface demineralization of teeth caused by bacterial acid from plaque. It is one of the most common diseases and a major cause of tooth loss. Dental caries has a multifactorial etiology involving diet, bacteria, time and a susceptible tooth surface. Key theories on the etiology of dental caries include the acidogenic theory, which proposes that acids produced by bacteria from carbohydrates lead to demineralization of enamel and dentin. Classification of dental caries is based on factors such as location, progression, surfaces involved, and tissue affected.