Downloaded 1,940 times






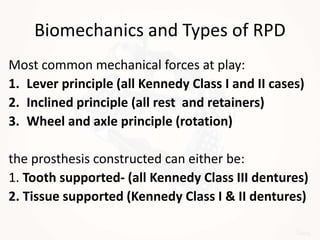
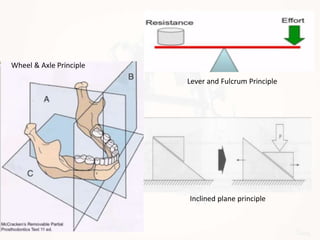
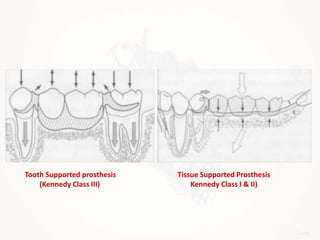





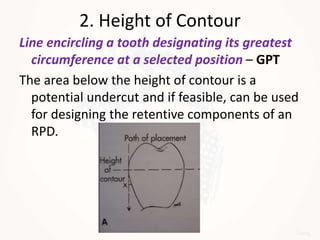

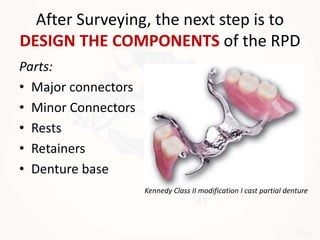










































This document discusses the design of removable partial dentures. It begins by classifying partially edentulous jaws using Kennedy's classification system. It then covers the basic considerations in design such as biomechanics, types of supports, and biological factors. The key steps in design are surveyed, including marking the path of insertion, height of contour, and undercuts. It describes the components of partial dentures including major connectors, minor connectors, rests, retainers, and the denture base. Specific clasp and retainer designs are covered for different clinical situations.



































































