Downloaded 11,498 times
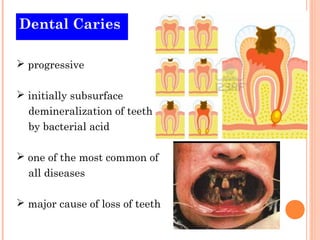
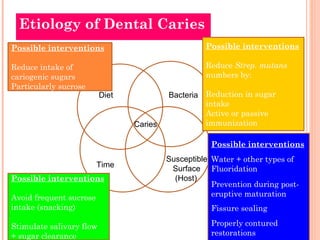
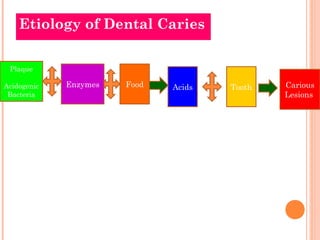
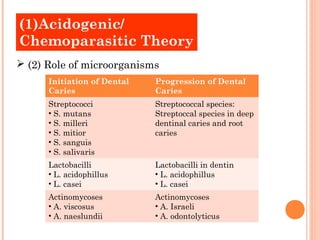
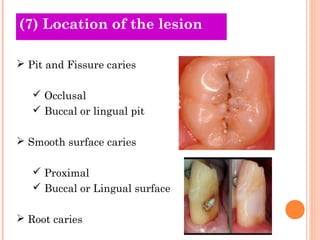
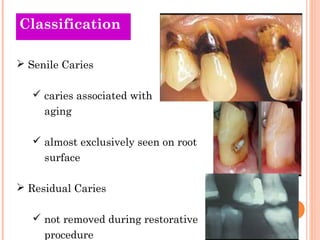

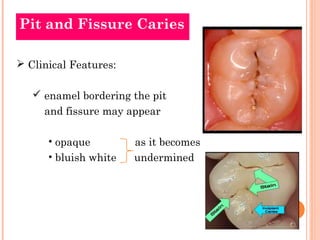
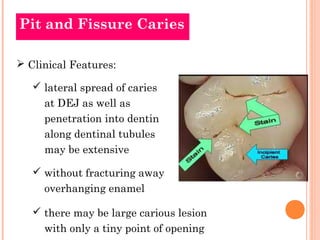
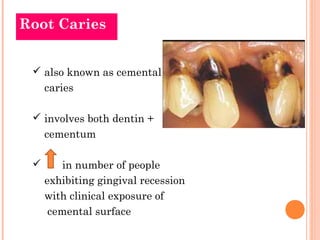

The document discusses dental caries, including its etiology and classifications. It provides details on: 1) Dental caries is a progressive, subsurface demineralization of teeth caused by bacterial acids that leads to tooth decay. 2) Old and new theories on the etiology of dental caries including the roles of carbohydrates, microorganisms, acids, and dental plaque in the acidogenic/chemoparasitic theory. 3) Classifications of dental caries including based on nature of attack, progression, surfaces involved, direction of attack, number of surfaces, GV Black classification, location, and tissues involved.













































































