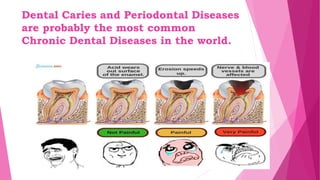
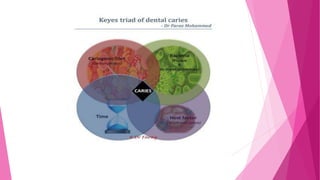
Dental caries is a chronic, multifactorial disease primarily caused by the interplay of host factors, microflora, and dietary substrate, particularly carbohydrates. The main microorganisms involved include Streptococcus mutans, which metabolizes sugars to produce lactic acid leading to tooth demineralization. The document discusses various theories of caries etiology, the role of dental plaque, the importance of saliva pH, and methods for diagnosis and prevention of dental caries.