Downloaded 106 times


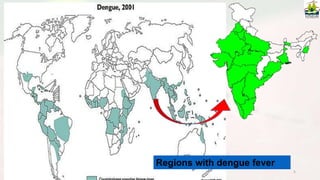
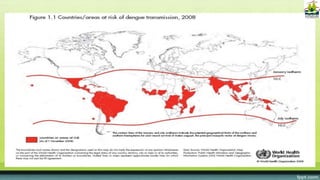


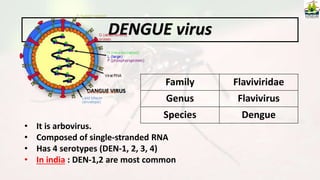
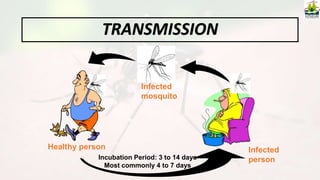
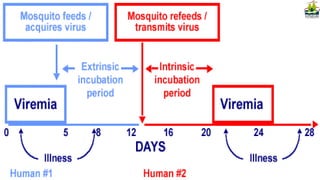

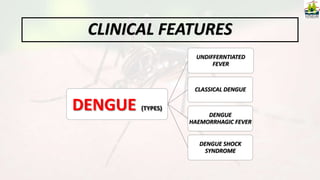







Dengue is a mosquito-borne viral disease transmitted by Aedes mosquitoes that can cause flu-like symptoms including fever, rash and joint pain. It is a major public health challenge in tropical and subtropical regions of the world with around 50 million cases estimated each year. The document outlines the causative virus, transmission, clinical features and management of dengue as well as prevention strategies focusing on mosquito control and community education.


































































































