
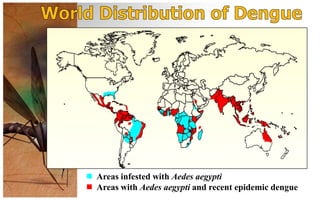
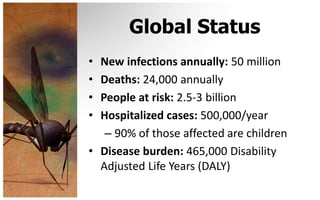

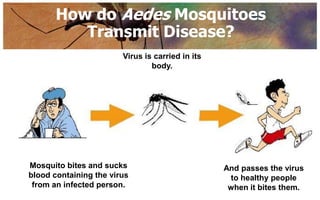



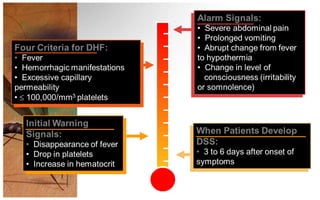
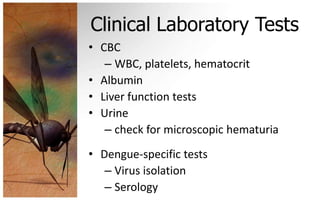







This document provides an overview of dengue fever, including its causes, transmission, global impact, and prevention. Some key points: - Dengue fever is a viral disease transmitted by Aedes mosquitoes, primarily Aedes aegypti. There are 4 types of dengue viruses. - It affects over 50 million people annually worldwide and is a major public health challenge in many tropical and subtropical countries, including the Philippines. - Transmission occurs when an infected mosquito bites a person and transmits the virus. There is typically an incubation period of 4-7 days before symptoms appear. - Symptoms range from mild fever to severe dengue hemorrhagic fever. Treatment depends on











































































































