Downloaded 246 times






















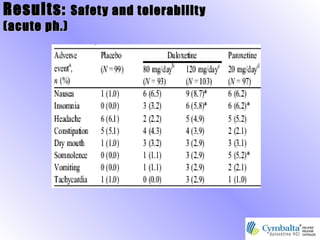






Cymbalta (duloxetine hydrochloride) is an FDA-approved selective serotonin and norepinephrine reuptake inhibitor (SNRI) for treating major depressive disorder (MDD). It affects emotional and physical symptoms of depression by correcting an imbalance of serotonin and norepinephrine in the brain. Clinical studies have demonstrated its efficacy in treating MDD with common side effects including nausea, dry mouth, and fatigue.





































































































