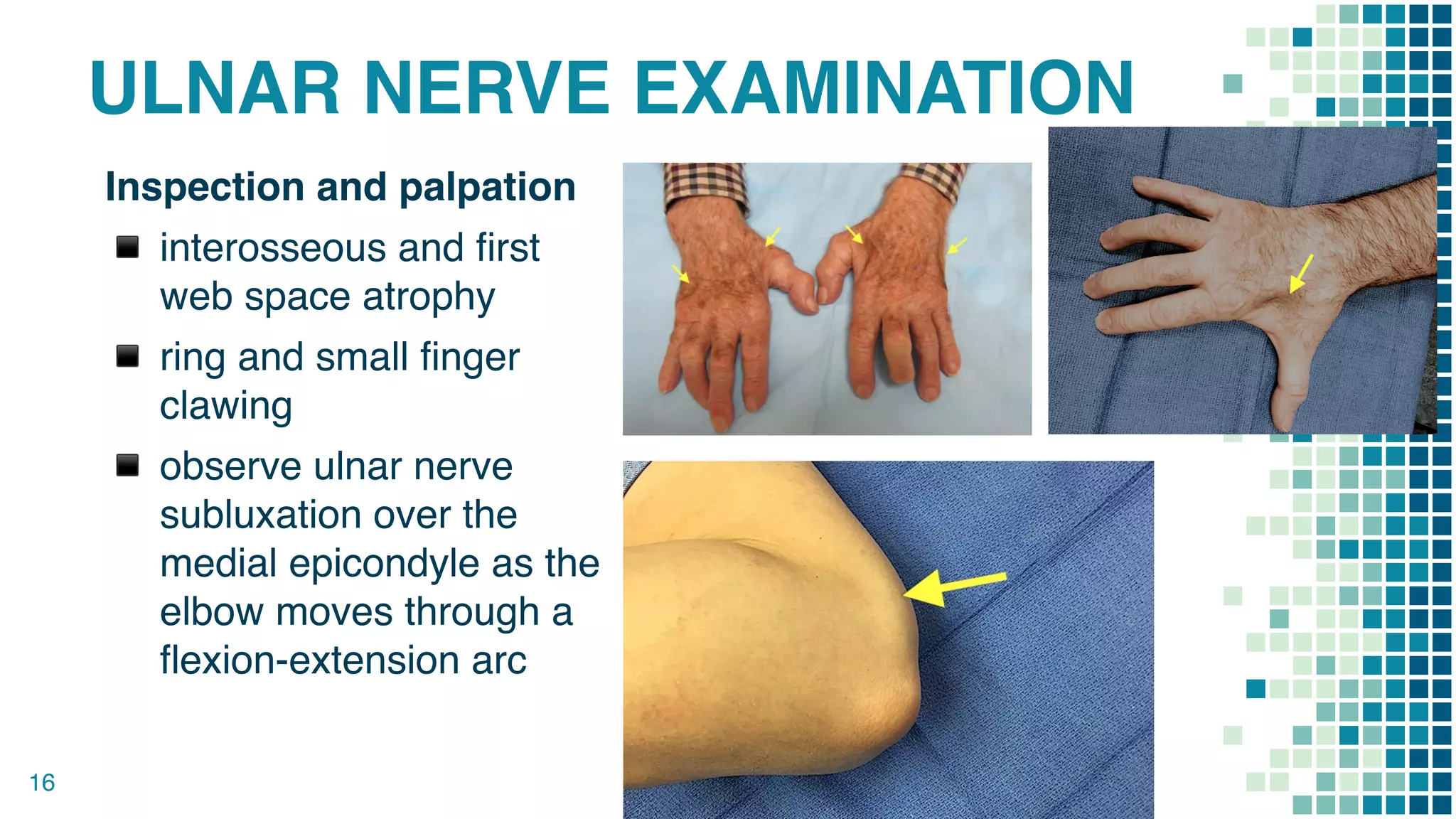
This document summarizes a case of cubital tunnel syndrome in a 40-year-old Thai Buddhist monk. He experienced numbness and tingling in his right ring and little fingers for 1 month after injuring his right elbow. Examination found signs of ulnar nerve dysfunction including clawing of the fingers. Imaging showed no abnormalities. He was diagnosed with cubital tunnel syndrome and scheduled for ulnar nerve decompression surgery.