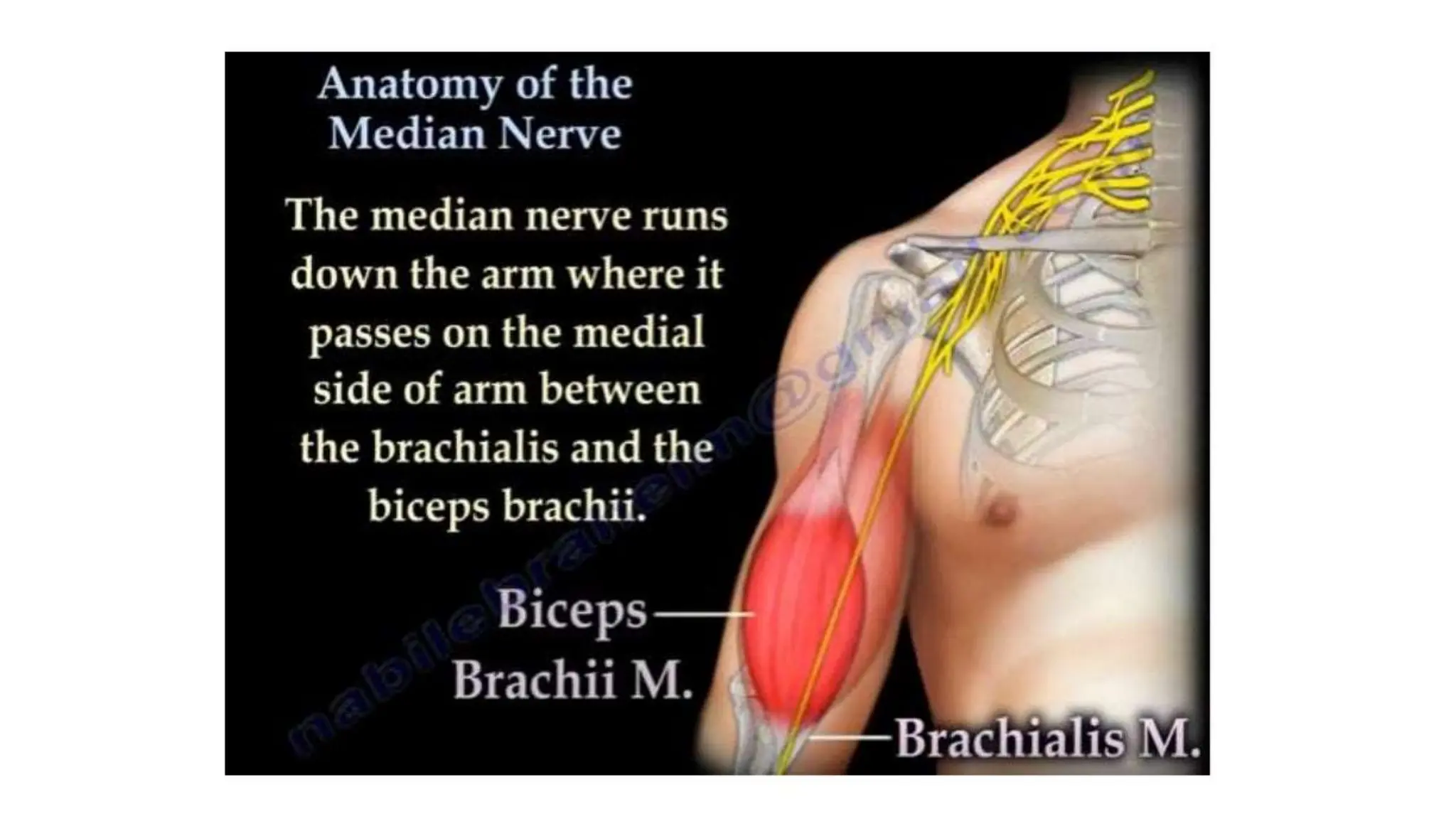
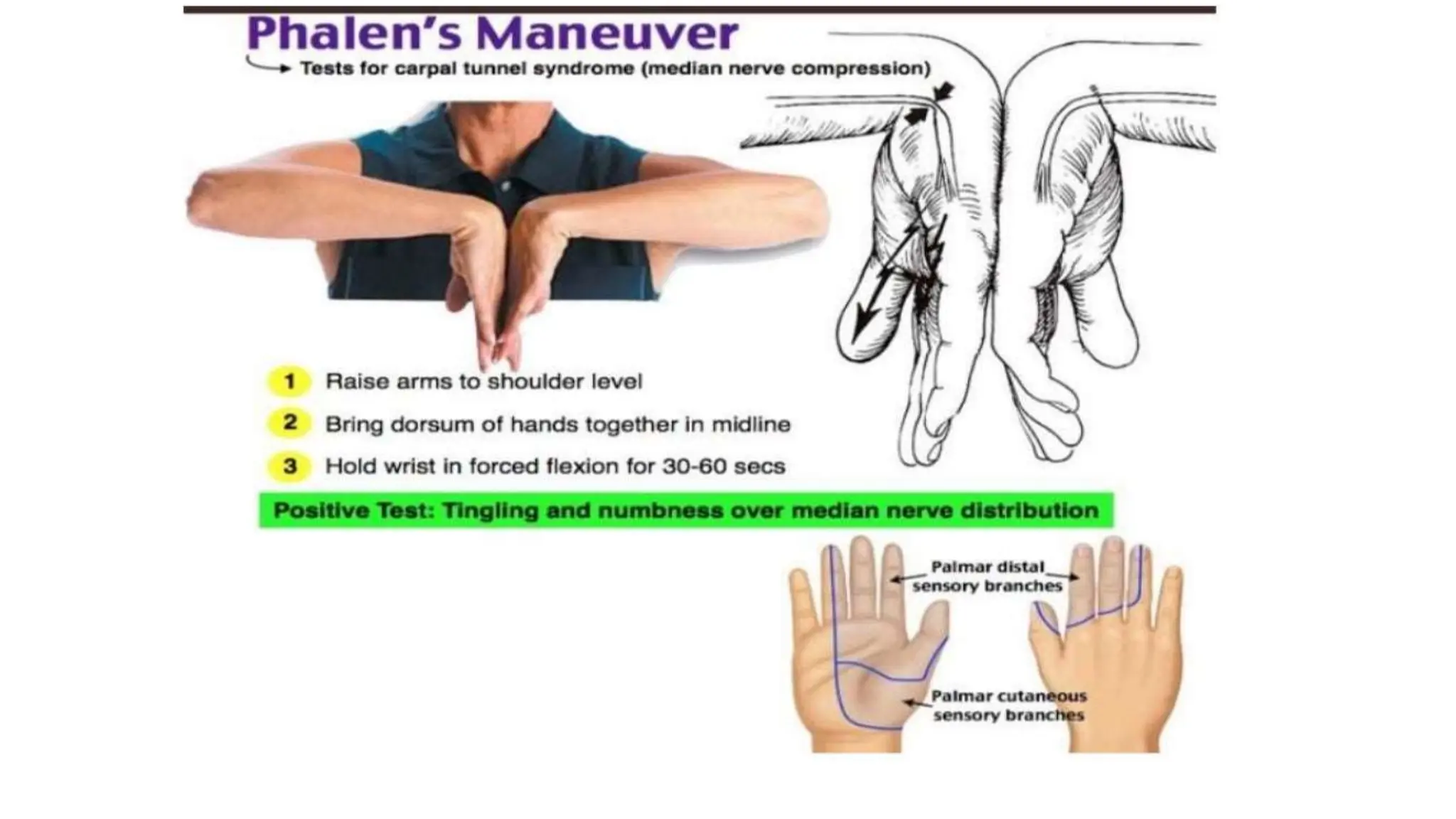
This document discusses the anatomy and injuries of the median nerve. It begins with the anatomy of the median nerve as it travels from the axilla to the forearm. It then discusses high and low injuries to the median nerve and their associated motor and sensory deficits. Examination techniques like the pronator teres assessment and Kleinert test are described. Median nerve compression syndromes like carpal tunnel syndrome are also covered. The document concludes with discussing indications for median nerve surgery, timing of surgery, and critical limits for delayed repair.




















































































































![GAIT and its different types[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gaitautosaved-240815185755-7939fafe-thumbnail.jpg?width=640&height=640&fit=bounds)






























