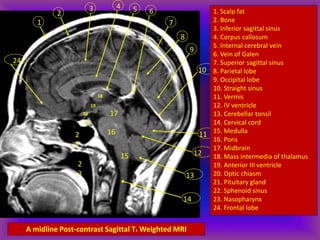
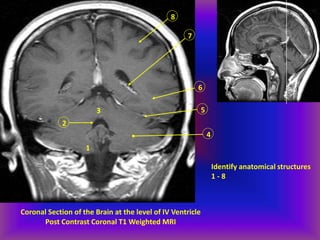
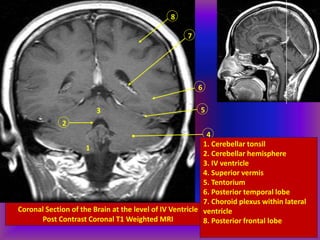
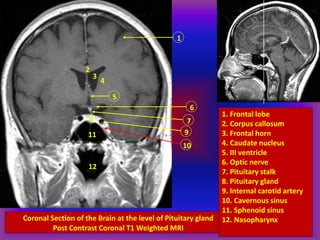
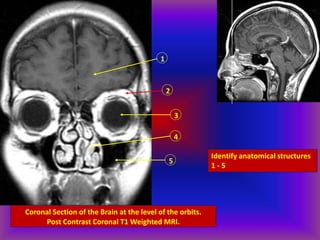
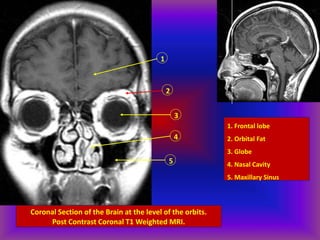
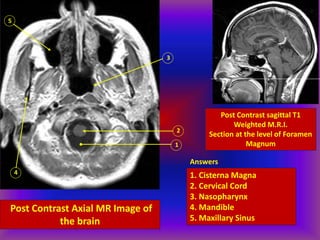
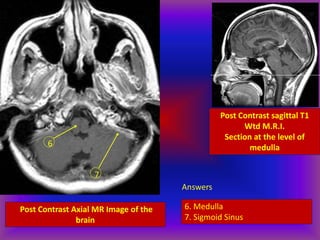
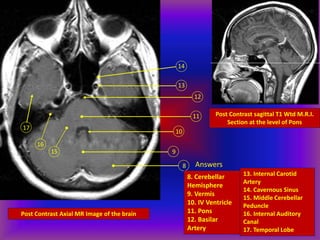
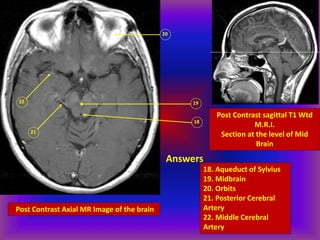
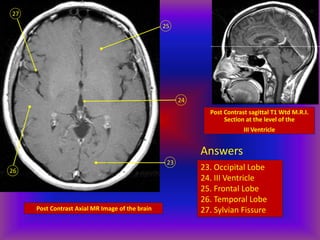
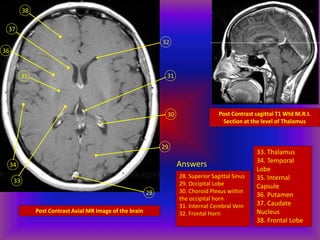
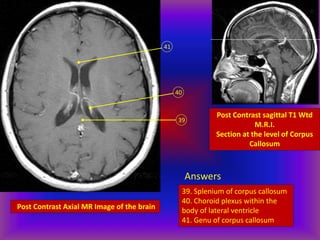
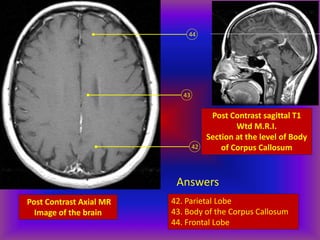
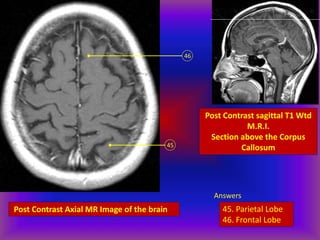
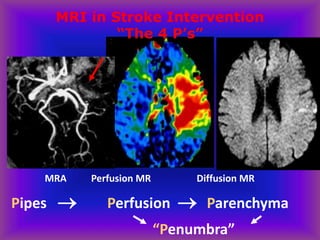
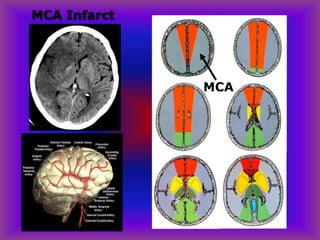
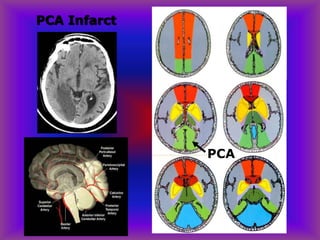
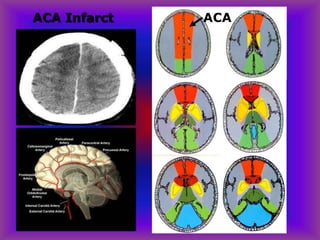
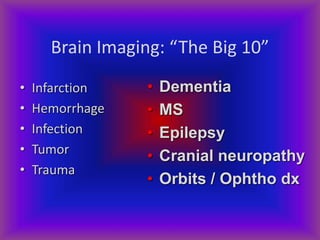
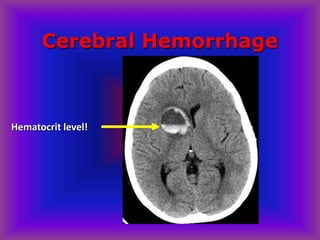
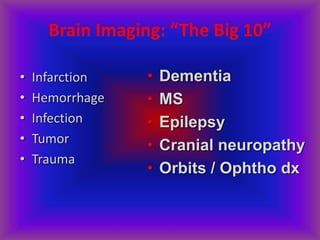
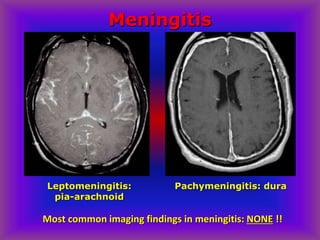
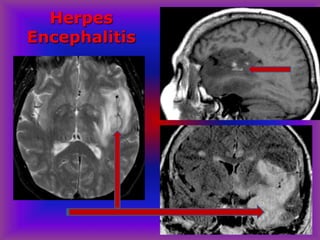
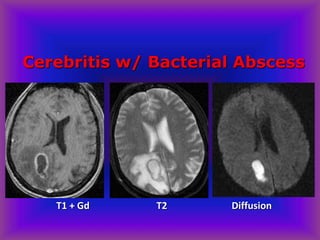
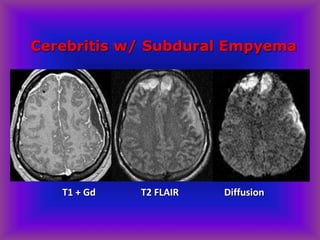
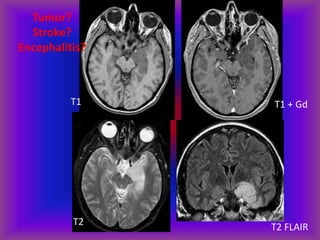
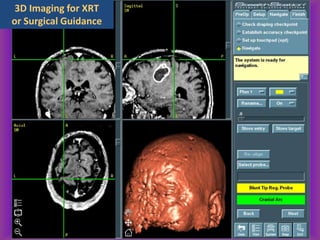
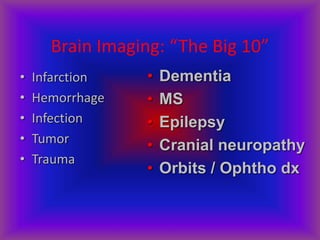
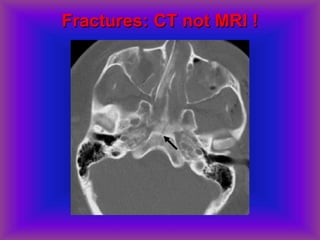
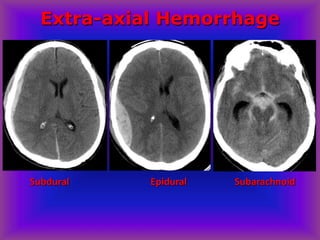
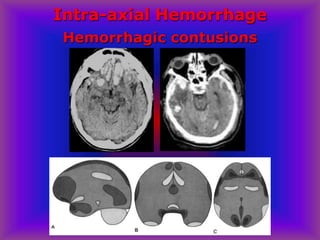
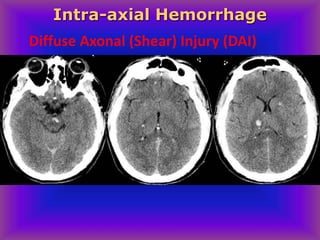
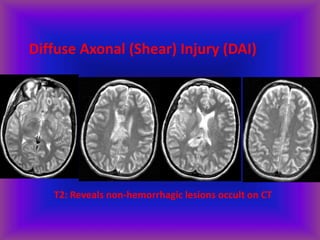
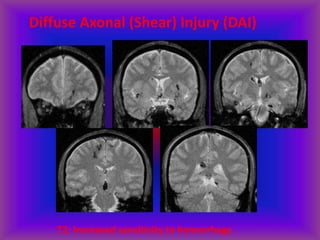
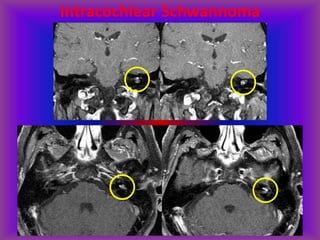
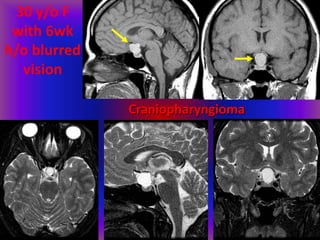
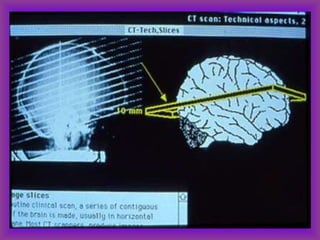
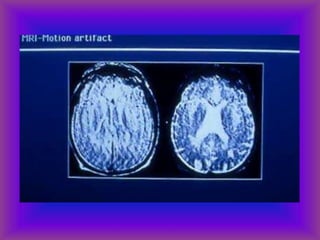
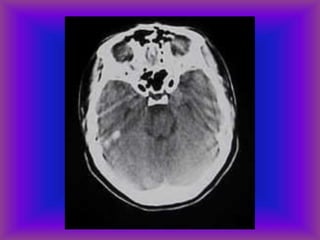
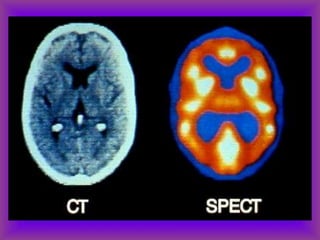
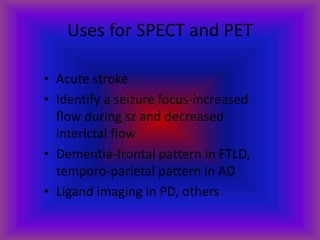
This document provides an overview of CT and MRI interpretation for various neurological conditions. It includes labeled images showing normal anatomical structures and examples of: stroke demonstrated on perfusion and diffusion MRI; hemorrhage on CT and MRI; brain infection; tumors; traumatic brain injuries; dementia; multiple sclerosis lesions; and epileptic foci. The document serves as an educational guide for medical students and residents to learn cross-sectional brain anatomy and recognize key imaging findings for common neurological disorders.





























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


