Downloaded 417 times


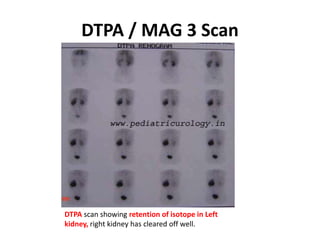
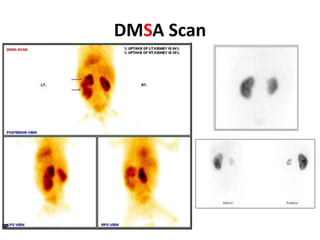
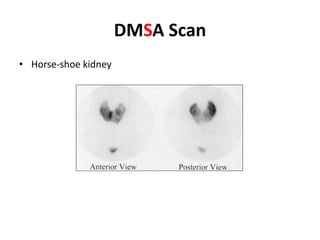
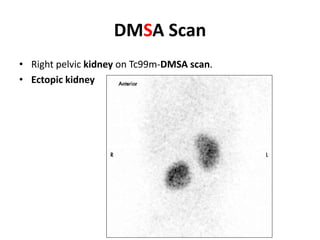
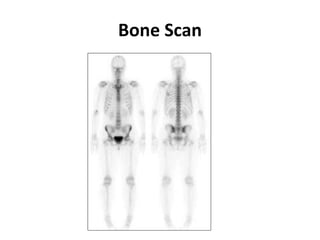
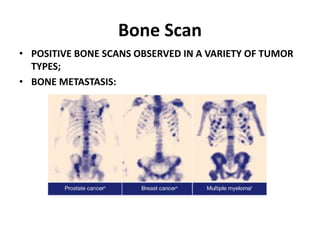
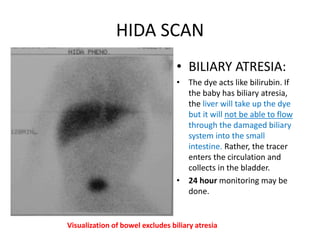
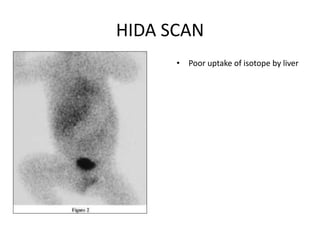


Diuretic renal scans use radioactive tracers like DTPA, MAG3, or LLEC to evaluate kidney function and rule out obstruction. DTPA/MAG3 scans provide information on renal blood flow, GFR, tubular function, and excretion. DMSA scans use Technetium99m to visualize renal cortex and assess renal scarring. Bone scans use Technetium99m HDP to detect bone metastases, tumors, and infections. HIDA scans use Technetium99m Hepatolite to evaluate gallbladder function and detect causes of jaundice like cholecystitis. Lung V/Q scans use radioactive gas and injections to detect perfusion mismatches diagnostic of pulmonary embolism











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





