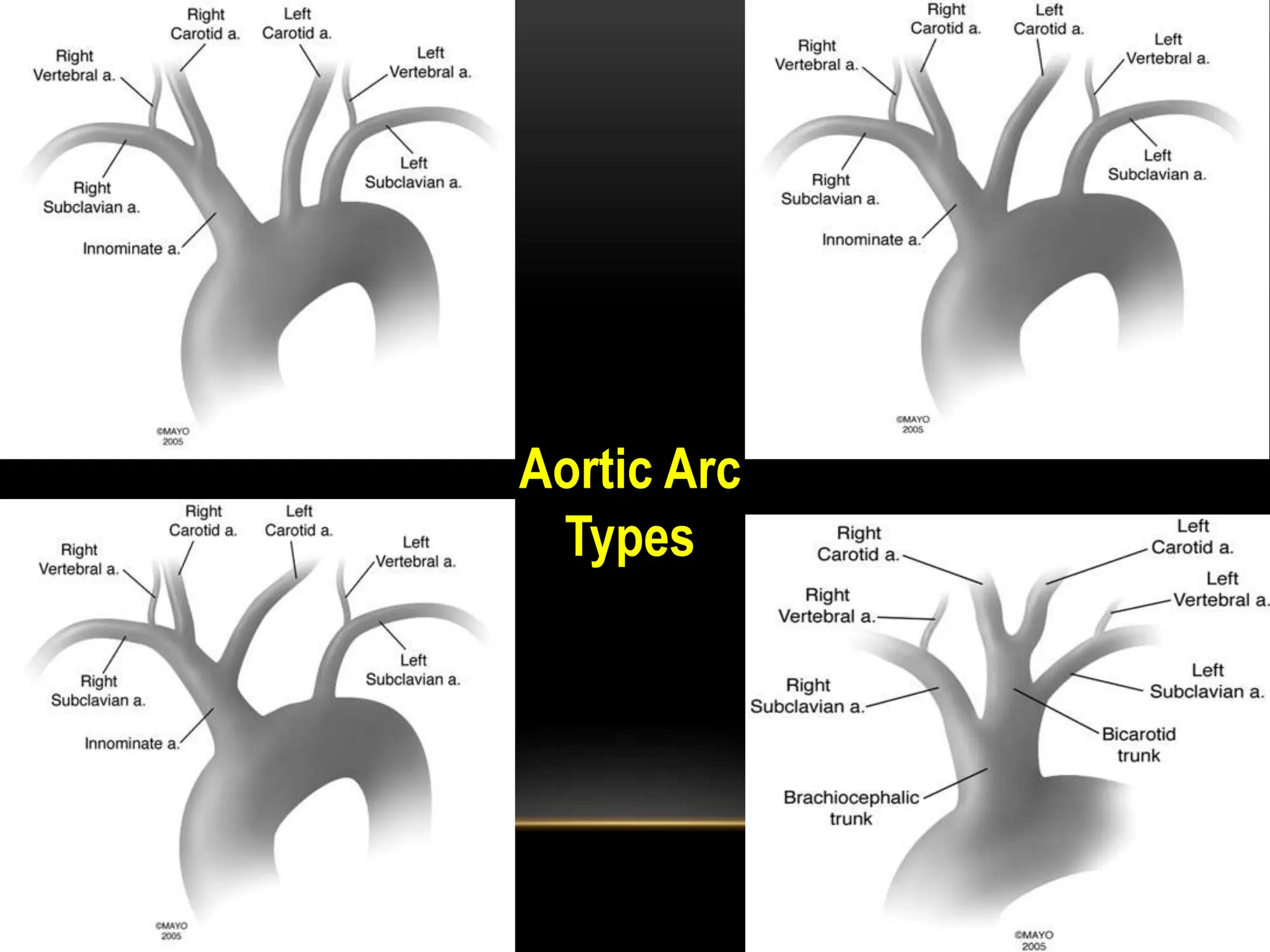
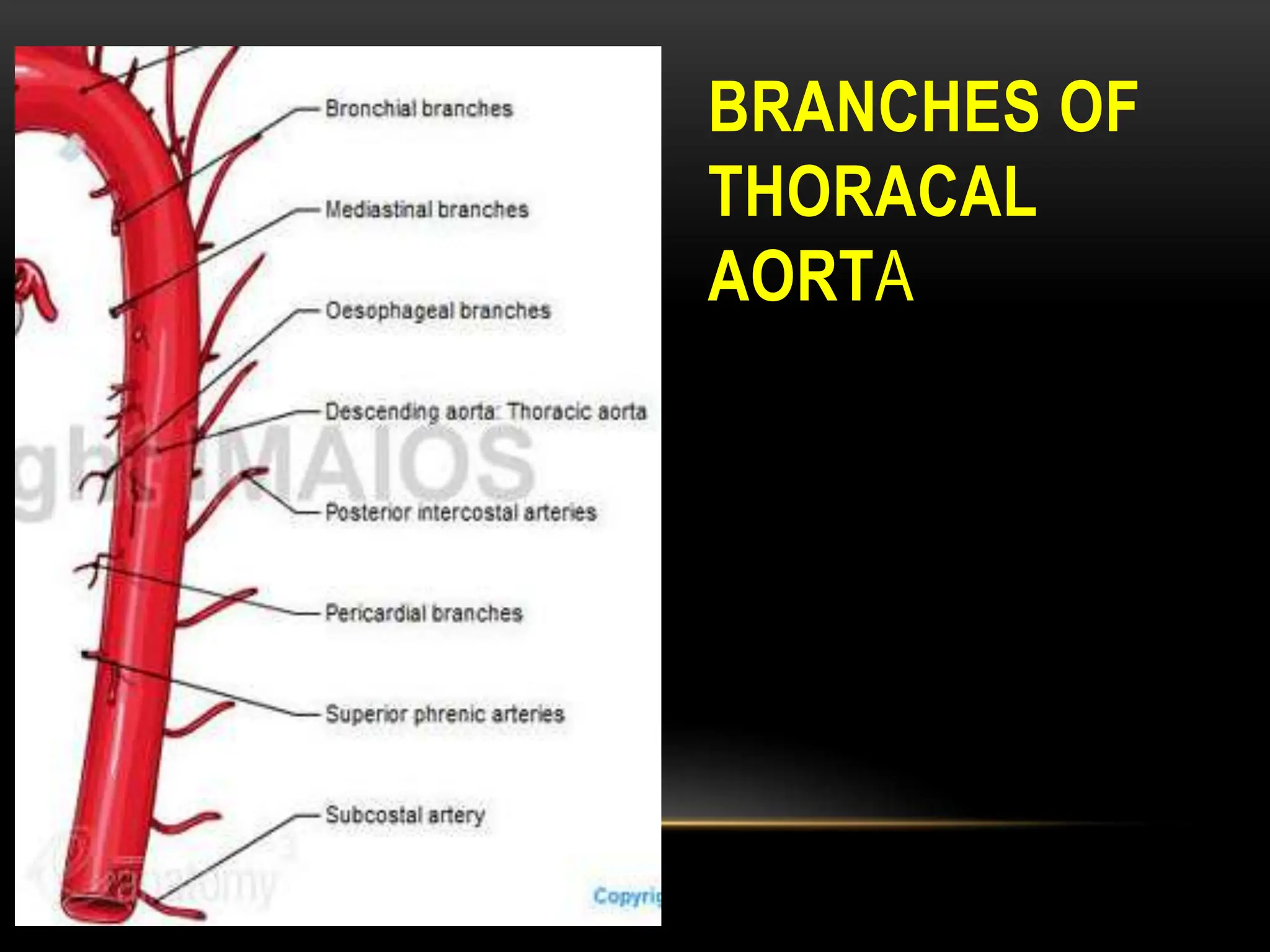
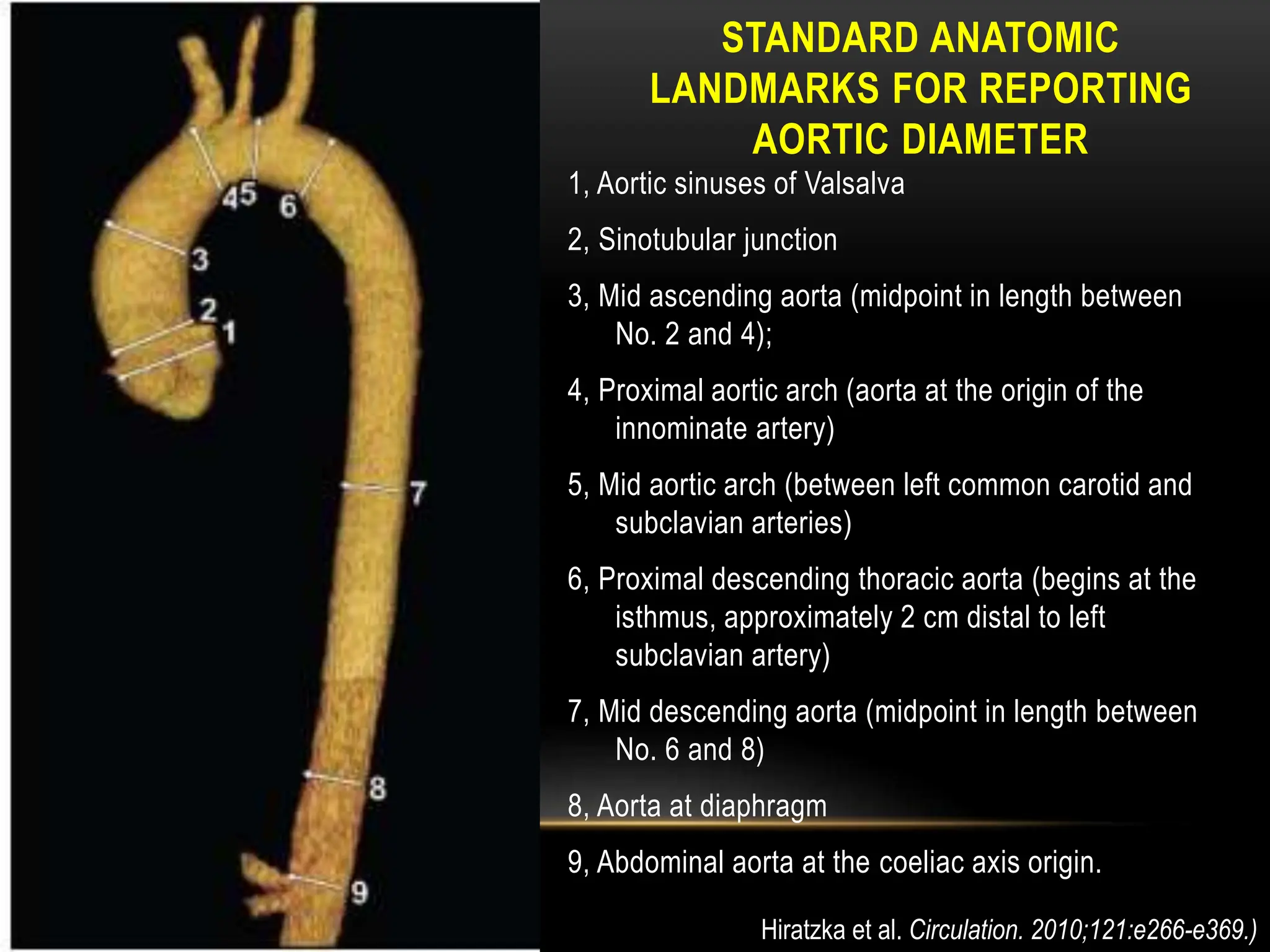
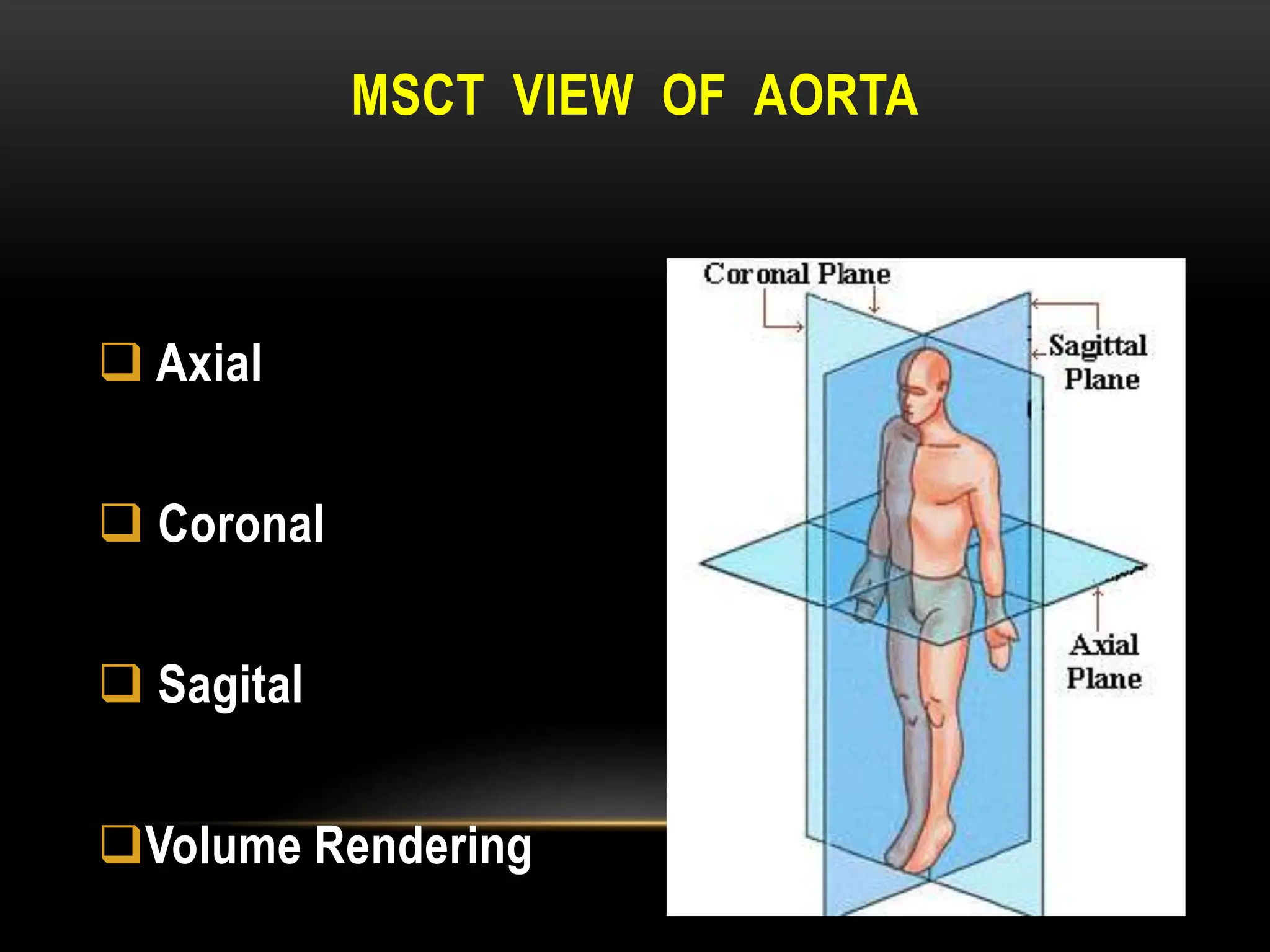
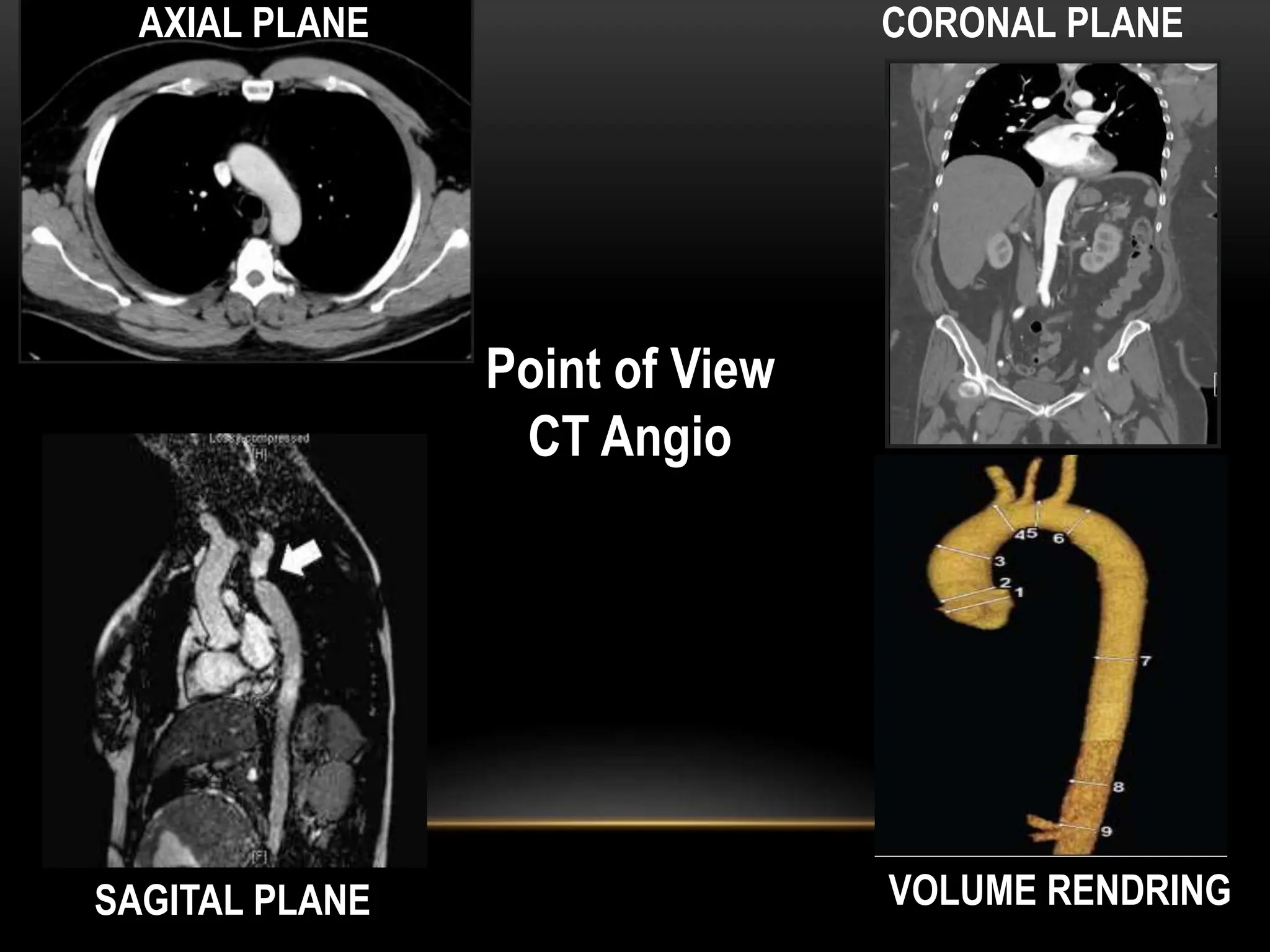
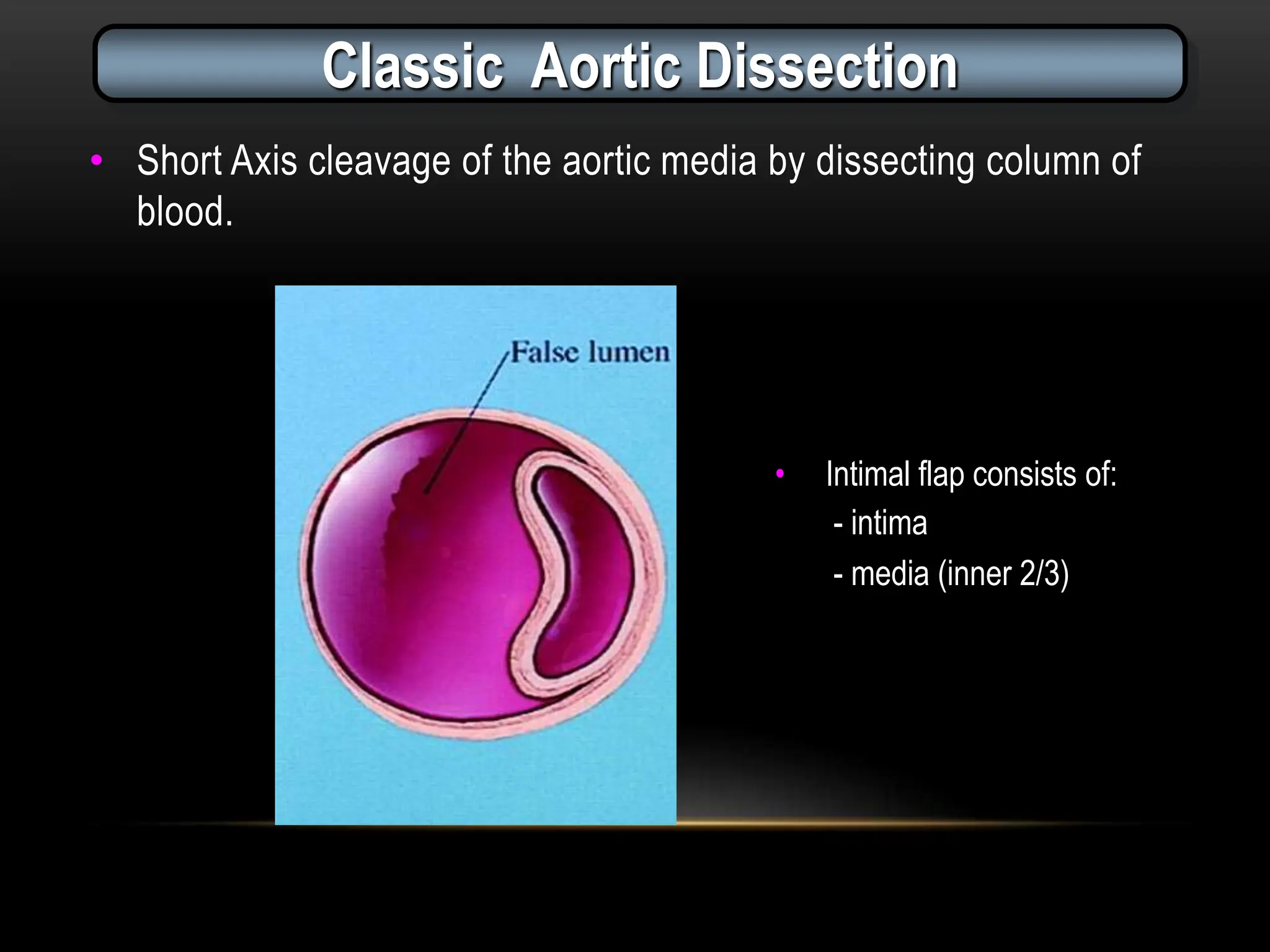
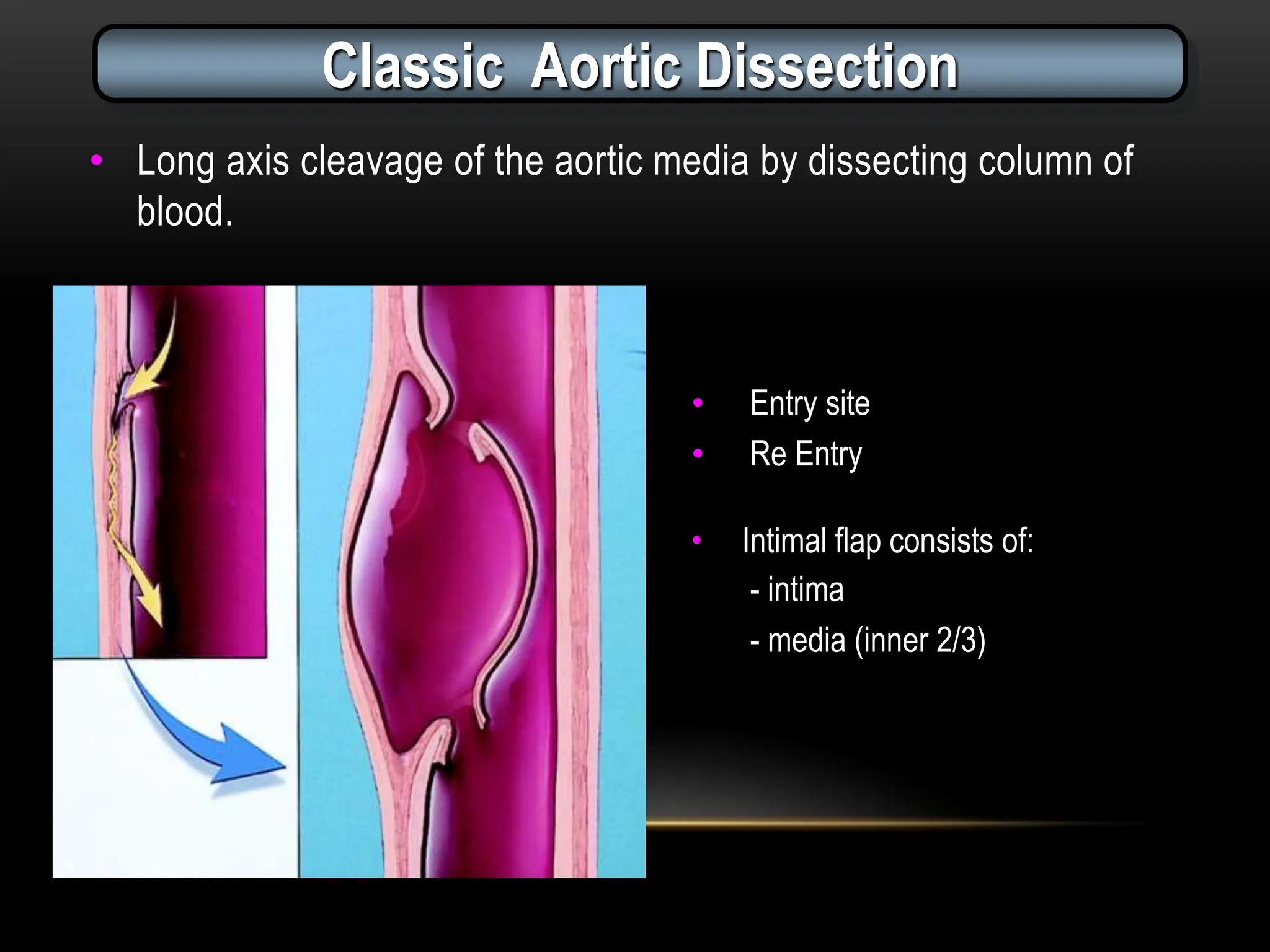
This document provides an overview of thoracic aortic anatomy, imaging modalities, and pathologies as assessed by CT imaging. It describes the normal anatomy and branches of the thoracic aorta, standard landmarks for measuring aortic diameter, and normal diameter ranges. It also details imaging appearances and classifications of thoracic aortic dissection, intramural hematoma, penetrating atherosclerotic ulcer, aneurysm, infection, and rupture. CT angiography is outlined as the preferred modality for evaluating thoracic aortic diseases due to its ability to provide axial, coronal, and sagittal views as well as 3D renderings.