• Leakage ofcerebrospinal fluid (CSF) through the
nasal cavity due to disruption of duramater, osseous
defect and nasal mucosa
• Anterior cranial fossa either via the frontal, ethmoid
or sphenoid sinuses or from the cribriform- plate.
• CSF leak can from the middle or posterior cranial
fossa and reaches the nasal cavity via the middle ear
cavity through the Eustachian tube.
• For CSF leak, pressure gradient should be greater
than healing tensile strength of the disrupted
tissues.
4.
• Paradoxical Rhinorrhoea
•Paradoxical rhinorrhoea is CSF leak into middle
ear cavity with intact tympanic membrane,
which flows into the nasopharynx via the
Eustachian tube.
• CSF leaks are persistent due to lack of WBC
platelets or fibrin.
5.
• Causes ofCSF Rhinorrhoea
1. Congenital: Meningocoele, meningoencephalocoele,
congenital skull base defects and congenital hydroceph-alus
2. Idiopathic
3. Trauma
Surgical: Intranasal surgery, endoscopic surgery and transcranial
surgery
Nonsurgical: Skull base fractures and open or penetrating injuries
4. Inflammatory
Erosive lesions like mucocoele, polypoidal diseases, cystic fibrosis,
fungal sinusitisPost infective hydrocephalus
5. Neoplasm :Neoplasm involving skull baseIntracranial
abnormalities causing hydrocephalus
6.
Traumatic
1. Accidental (80%):Immediate/delayed
2. Surgical: (Acute/delayed)
a)Trans-sphenoidal hypophysectomy
b) Acoustic neuroma surgery
c) Endoscopic nasal/sinus surgery
d) Skull base surgery
7.
B. Non-traumatic
High pressure(45%)
a) Tumours (85%)
Direct mechanism: Rare
Indirect mechanism: More common. Due to increase in intracranial
pressure
b) Hydrocephalus (15%)
Obstructive type
Communicating type
Normal pressure (55%)
Congenital anomalies:
Prolongation of subarachnoid space along olfactory nerve and pituitary
Maldevelopment of cribriform plate or diaphragm sellae.
Skull base neoplasm: Nasopharyngeal carcinoma, sinonasal malignancy
Skull base erosive process: Osteomyelitis Idiopathic
Post-traumatic CSF rhinorrhoea develops within 48 hrs in55% cases and
by 1 week in 70% cases.
8.
• Causes ofdelayed post traumatic leak
Delayed increase in intracranial pressure
Lyses of clot plugging the leak
Resolution of soft tissue edema
Maturation and contraction of wound edges
Herniation of duramatar through fracture line
9.
IATROGENIC OR POSTSURGICAL CSF
RHINORRHEA
• The risk of CSF leak after ESS is reported to be around
0.5%.
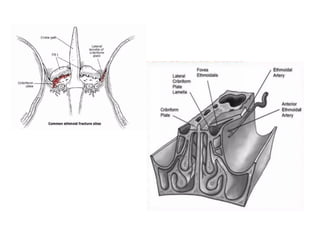
• The most common site of injury during ESS is the lateral
cribriform lamella, mainly on the right side.
• Aggressive middle turbinate retraction or resection may
be associated with LLCP injury
• The other common sites of injuries include the posterior
fovea ethmoidalis, sphenoid sinus.
• Powered instrumentation is invariably associated with
greater removal of tissue; as a result, the resultant skull
base defect may be quite extensive.
11.
CSF LEAKS ASSOCIATEDWITH TUMORS
• Tumours causing substantial erosion of the skull
base may present with CSF rhinorrhea.
• Occasionally where tumour shrinkage occurs, for
example during induction chemo-therapy, CSF leaks
may also occur.
• The closure of the CSF leak is part of the surgical
treatment of the tumour
• For the closure to be successful it is important for
the margins of the CSF leak to be clear of tumour,
particularly in malignant disease.
12.
CONGENITAL CSF LEAKS
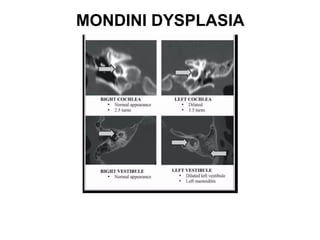
•Congenital abnormalities of the inner ear such as the Mondini
Dysplasia may present with substantial CSF leaks where the
CSF has only briefly transversed the perilymphatic space.
• Such leaks, in addition to presenting as hearing loss or
recurrent meningitis, may also present with CSF otorrhea or
CSF oto-rhinorrhea
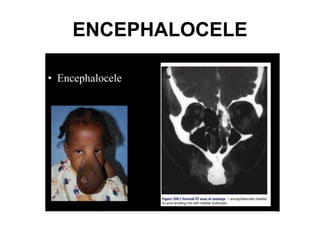
• Congenital CSF leaks in association with encephalocele or
meningoencephaloceles are uncommon.
• These are well diagnosed on MRI and Brain tissue contained
within the encephalocele is invariably non-functioning and can
be removed as part of the surgical procedure.
SPONTANEOUS CSF LEAKS:
•sometimes described as 'idiopathic'
• middle-aged women with a raised body mass index.
• represent a variant of benign intra-cranial hypertension.
• radiological features of increased intra-cranial pressure such as
an empty sella, enlarged ventricles or diffuse erosion of the
skull base may be seen
• Herniation of the meninges and brain, often with CSF leakage
most often occurs
❖ in the lateral recess of a well pneumatized sphenoid,
❖ in the area of the lateral lamella of the cribriform and
❖ in the ethmoid roof.
These may be multiple sites of weakness of the skull base.
16.
• It couldbe postulated that in patients with occult elevated CSF
pressure, the CSF leak may serve as a release valve that
decompresses the elevated pressure
• Identification of 'spontaneous’ as the likely aetiology of the leak
pre-operatively is helpful in counselling the patient.
• Spontaneous leaks are most likely to recur and the success rates
for endoscopic closure are worse than for other aeteologies.
• CSF leaks in the lateral recess of well pneumatized sphenoid
sinuses may be best approached by the transantral
transpterygoid approach described by Bolger.
• Post operatively, the elevated intra-cranial pressure may be the
repair with generally good results. The most likely helped by
oral acetazolamide.
17.
• ommaya's Theoryof Focal Atrophy
• Normal content of sella/cribriform area may
undergo ischaemic necrosis resulting in empty
space filled with CSF, which subsequently
results in pressure pulse of this CSF. Pouch
causes erosion resulting in CSF leak.
18.
Symptoms
Persistent rhinorrhoea followinghead injury or
surgical trauma.
unilateral or bilateral
Unilateral watery nasal discharge most common
continuousor intermittent.
Watery discharge is aggravated with heavy work
or strain or with change of position of the head
such as getting up suddenly from the supine
position.
19.
• Headache
• relievedby straining/reclining is low pressure
headache due to excess CSF leak in normal
pressure.
• Headache relieved by rhinorrhoea is high
pressure headache.
• Headaché can be due to raised intracranial
tension, meningitis or may indicate the
presence of pneumocephalus.
20.
• Hyposmia andanosmia and/or parosmia.
• Salty taste in the mouth.
Repeated attacks of meningitis especially with
Pneumococcus
Unexplained weight loss may be suggestive of
neoplasm.
21.
• Differential diagnosiswith allergic rhinitis
CSF leak appears súddenly without, warning. CSF
leak uncontrollable and cannot be sniffed back.
Nosneezing/nasalcongestion/lacrimation/
response to antihistamines.
CSF does not contain mucus, so does not stiffen
thehandkerchief.
CSF has a salty taste.
22.
• Reservoir sign:Place patient in supine position
for sometime then bring to upright position
with neck flexed. Sudden gush of clear fluid is
suggestive of CSF leak. The reservoir sign is the
ability of a patient to voluntarily produce CSF at
will by correct positioning thehead.
23.
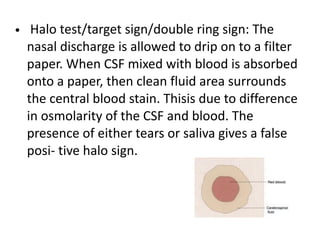
• Halo test/targetsign/double ring sign: The
nasal discharge is allowed to drip on to a filter
paper. When CSF mixed with blood is absorbed
onto a paper, then clean fluid area surrounds
the central blood stain. Thisis due to difference
in osmolarity of the CSF and blood. The
presence of either tears or saliva gives a false
posi- tive halo sign.
24.
• Handkerchief test:The nasal discharge is
alloweddrip on to a handkerchief; if the wet
handkerchief dries without stiffening then it is
suggestive that the rhinor- rhoea is caused by CSF.
CSF does not stiffen the hand- kerchief as does not
contain any mucus or albumin.
• If leakage with upright head or a backward tilted
head, then defect in cribriform plate/ethmoid roof/
frontal sinus. Internal jugular vein compression can
increase CSFleak. Leakage only on tilting the head
forward, then defect in sphenoid sinus (tea pot) or
via Eustachian tube.
25.
• INVESTIGATIONS
• Nasalendoscopy
• Glucose oxidase test
• Chloride estimation in nasal discharge
• Plain X-ray
• B-Trace protein
• B,-Transferrin assay
• CT scan
• CT scan cisternography
• MRI scan T,-weighted images
• Non-ionic contrast computed tomography cisternography
(NCTC)
• Intrathecal fluorescin
• Positron emissic tomography (PET)
• Tests for olfaction and document for medicolegal reasons
26.
• Nasal Endoscopy:
•Can be used for the diagnosis of CSF leak and if unable
to localize the site, the patient is asked to perform
Valsalva manoeuvre, which results in a sudden gush of
CSF from the leak in a suspected area.
• The leak can be from one of the following site or
combination
• Cribriform plate
• Middle meatus :leak is in anterior ethmoid
• Superior meatus: Leak is in posterior ethmoids
• Sphenoethmoidal recess: Leak is in sphenoid
• Eustachian tube orifice: Leak is through middle ear
27.
Glucose Concentration ofNasal Discharge:
• When the nasal discharge, suspected of cerebrospinal fluid, is
applied to glucose oxidase impregnated test strips, a colour
change in the strip is suggestive of cerebrospinal fluid.
• Concentration more than 30 mg/mL in the discharge is
confirmatory of CSE leak.
Drawbacks
• Contamination of blood.
• Presence of tears and nasal mucus gives false-positivetest.
• Presence of bacterial meningitis give a false-negative test.
Chloride Assay in Nasal Discharge:
Chloride in CSF fluid is about 120 mEq/L, which is higher than
serum range of 98-112 mEq / L.
An elevated chloride value an unknown sample of dripping from
the nose is highly suggestive of CSF.
28.
• Beta TraceProtein
• Beta trace protein is found in cerebrospinal fluid, heart
and serum.
• Sensitivity and specificity are not as high as ẞ,
transferrin.
• Elevated with renal insufficiency, myocardial infarction,
cerebral infarcts and some CNS tumours.
• If serum level is less than 1.0 mg/L then nasal discharge
with a concentration of more than 2.0 mg/L is positive
for the presence of cerebrospinal fluid
• concentration of less than 1.5 mg/L is not likely to
contain cerebrospinal fluid..
29.
• β2transferrin hasnow emerged as the preferred
biochemical marker of CSF.
• Because β2-transferrin is a reliable marker of CSF, it
has been proposed that a negative β2-transferrin test
result in a patient with a suspected CSF leak may be
sufficient justification for not performing additional
invasive procedures
• Detection of βTP has 100% sensitivity and specificity
in cases of confirmed CSF rhinorrhea
30.
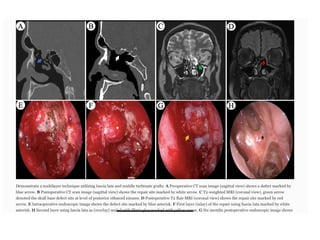
• HRCT andMRI Cisternography
• HRCT:
• Thin-section axial and coronal scans of cranial and facial
region, including all the paranasal sinuses and petrous
temporal bones.
• Demonstrate fractures and bone defects well than MRI.
• Also show protruding soft-tissue (meningoencephalocele )
through the bony defect , and demonstrate focal fluid
accumulation in the sinuses (ethmoid, frontal, sphenoid,
and maxillary sinuses), and pneumocephalus in some
cases.
• CT imaging detects the fluid poorly and may not identify
exact site of leak when there are multiple fractures or
dehiscence
31.
MRI:
• Thin-section MRcisternography is performed with heavily T2-weight
• The intrathecal injection of 0.5 ml of gadopentetate dimeglumine,
diluted in 3-5 ml of CSF, for MR cisternography has been found to
have high sensitivity and specificity for detection of active CSF
rhinorrhea.
• Although prone position is uncomfortable, it may improve
rhinorrhea detection rate.
• Could demonstrate a defect in the cribriform plate and herniation
of meninges and brain tissue with adjacent CSF into the bone
defect.
• CSF rhinorrhea may be difficult to differentiate from sinusitis on
axial images. fluid-attenuated inversion recovery (FLAIR) imaging is
very helpful in differentiating CSF from non-CSF fluid
34.
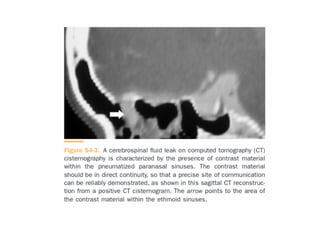
CT CISTERNOGRAPHY :
•Cisternography with an intrathecal injection of
nonionic iodinated myelographic contrast medium
usually localises the CSF leak.
• Increase in HU values by more than 50% in post-
cisternographic image indicates leak
• This is a useful single investigation in resource-
constrained situations, especially in active leak
• CT cisternography may have a problem in detecting
low-flow rhinorrhea or rhinorrhea with hair line
communication, Another limitation of this
procedure is its invasive nature.
37.
RADIONUCLIDE CISTERNOGRAPHY:
• Radioactiveisotopes can be introduced into the CSF by
means of lumbar or sub-occipital puncture.
• Head images are acquired 2, 6, 12, and 24 hours after
injection of the isotope
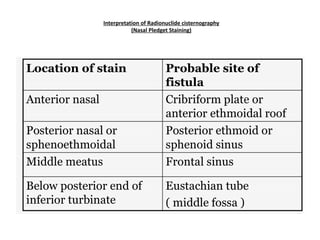
• Another option is to introduce nasal pledgets in various
high-risk areas. These pledgets can be analyzed for the
presence of the tracer.
• Radionuclide cisternography is used only when occult CSF
leak is suspected and imaging does not show a definite
skull base defect.
• Do not adequately localize the defect, can contaminate
extracranial tissue,False-positive results are seen in as high
as 33% patients.
FLUORESCEIN CISTERNOGRAPHY:
• Non-ophthalmicsolution of 0.1 ml of 10% fluorescein is diluted in
10 ml of CSF and injected into the subarachnoid space over a
period of 10 minutes.
• Nasal endoscopy is performed approximately 30 minutes after an
intrathecal injection.
• The intrathecal sodium fluorescein has been found to be useful in
diagnosing , localising and evidencing postop success rates of CSF
rhinorrhea.
• Complications such as seizures are reported .
• The side effects, if seen, are transient in dilute concentration. These
complications can be further minimized by careful lumbar puncture
and slow administration of the dye.
• The US Food and Drug Administration have not approved the use of
intrathecal fluorescein for the diagnosis or treatment of CSF
rhinorrhea.
40.
CSF OTORRHEA
• Cerebrospinalfluid (CSF) otorrhea -Presence of
CSF within the confines of the temporal bone
• Defect in the dura -abnormal communication
between subarachnoid space and aircontaining
space of temporal bone
41.
• The causesof CSF otorrhea
• Trauma (temporal bone fracture)
• latrogenic( skull base surgery)
• Neoplastic
• Infectious
• CongenitalSpontaneous CSF otorrhea - Not
related to the above-mentioned causes
42.
• The mostcommon locations are
• lateral to the cribriform plate
• along the floor of the middle fossa from the tegmen
tympani to the lateral surface of the sella turcica.
• infrequently located in the posterior fossa plate of
the Temporal bone between the sigmoid sinus and
bony labyrinth and in the region of the jugular
foramen.
• There may be an increased incidence of the AG on
the right side of the skull-right side predominance of
the venous system.
43.
• Pathophysiology ofspontaneous CSF otorrhea
• Congenital defect theory (Rao A et al, 2005) -
Defects of the middle fossa tegmen enlarged
(constant CSF pressure) Dural herniation
thinning out-csf leak
• Arachnoid granulation theory( Gacek, et al
1999) - Abnormally located arachnoid
granulations Minor CSF reservoirs. Abnormal
locations decreased return to the venous
systems Thinning and erosion of bone
44.
• Clinical presentation
•Young children:h/o recurrent Meningitis-
SNHL( Congenital anomalies)
• Obese middle-aged or elderly women:
Decreased hearing or aural fullness with middle
ear effusions
• Persistent serous or clear discharge after
myringotomy
45.
• management
• Restrictednose blowing
• Avoidance of straining- Bed rest and head
elevation of 30 degrees
• Use of antiemetics, antitussives and stool
softeners
• Diuretics and fluid restriction
• Lumbar drain
46.
• Surgical intervention
•Various approaches-
• Transmastoid & translabyrinthine- Middle fossa
craniotomy
• Materials used to correct bony defect: - Bone,
cartilage, fascia, abdominal fat, silastic and
various combinations of autologous tissues.
47.
• Transmastoid- Preferredapproach for most
patients.Extracranial visualization of middle
and posterior fossa without damage of
intracranial tissues
• Translabyrinthine approach - For patients with
no hearing - Remove all middle ear structure
Occlude Eustachian tube with bone wax,
muscle and fascia Obliteration of middle ear
with muscle or fat and close EAC
TREATMENT OF TRAUMATICCSF RHINORRHEA
• Most traumatic CSF leaks stop on their own-
• 35 % leaks stopped within 24 hours
• 68 % within 48 hours
• 875 % within 1 week
51.
Conservative treatment
• Position- elevate head 30-45° for cranial leaks
• Avoid sneezing, coughing, straining
• Monitor carefully for neurological deterioration-
meningitis or pneumocephalus
• Antibiotics - for prevention of meningitis
• Pharmacological adjuvants - Diamox, Frusemide
• Subarachnoid drainage through lumbar catheters
52.
Lumbar drain
• Indicatedif positioning and diamox alone does not significantly
decrease CSF leak within 24 hours
• Rationale - Granulation tissue can seal the fistula provided that
the leak has stopped
• CSF drainage to be continued for 3 - 5 days after stoppage of leak
to allow healing
• Complications -
• Over drainage of CSF - pneumocephalus, intracranial
haemorrhage
• High CSF protein concentration - Blockage
• Meningitis
• Broken catheter tip
• Dural-cutaneous fistula
54.
INDICATIONS FOR SURGICALINTERVENTION
• Traumatic or post-operative leaks that recur or persists even after
2 weeks of conservative management.
• High pressure leaks that act as safety valve for hydrocephalus.
• Leaks associate with erosion, destruction, disruption or
combination of these at skull base and para nasal sinuses.
• Leaks associated with congenital anomalies.
• Recurrent attacks of meningitis.
• Radiological appearances that indicate a low probability of
natural dural repair-
• Erosion, destruction or severe comminution of skull base or
sinuses
• Intracranial spikes of bone
• Soft tissue between the bony edges
55.
General principle
• Treatmeningitis and rule out hydrocephalus
before embarking on any surgical procedure
• Careful identification of the site and extent of
the dural defect
• Dissection of the bony and dural defect
• Direct dural repair if possible
• Closure using a graft(‡ glue), if direct dural repair
is not possible
56.
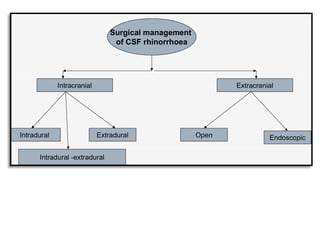
TRANSCRANIAL TECHNIQUES
• Aftercraniotomy, the defect site is identified, and then a
tissue graft is placed to close the defect.
• Fascia lata grafts, muscle plugs, and pedicled galeal flaps
may be used. A tissue sealant, such as fibrin glue, may be
used to hold the grafts in position.
• Access to the cribriform plate region and roof of the
ethmoid requires a frontal craniotomy:
• extended craniotomy and skull base techniques with even
greater brain compression provide access to the sphenoid
sinus defects.
• Despite direct access to the skull base defect, failure rates
are quite high , hence extra-cranial techniques are preferred
57.
EXTRACRANIAL APPROACH
OPEN
• viaan external ethmoidectomy for access to the
cribriform plate and fovea ethmoidalis
• transmastoid for defects in the tegmen and petrous
temporal bone
• transseptosphenoidal for access to the sphenoid sinus
• via a coronal or eyebrow incision to the frontal sinus using
an osteoplastic flap.
• method of choice for accessing most leaks of the posterior
wall of the frontal sinus
• minimises the incidence of intracranial complications
58.
ENDOSCOPIC
• OVERLAY
• UNDERLAY
•BATH PLUG
• MULTIPLE
• GASKET SEAL TECHNIQUE
➢These techniques are based on the position of
placement of graft , Layers of graft
59.
• Different techniquesand materials are adopted in the endoscopic
transnasal repair, starting with complete or partial trimming of
the middle turbinate (MT) to get better access and visualisation,
and the intraoperative identification of the leak site has been
done.
• The mucosa is completely stripped away from the defect site for
at least 5 mm in all directions.
• The bony projections near the defect were drilled out and
regularised for better graft placement and taken up by the bed of
the leak site.
• Superior turbinate resection is not routinely necessary for access.
• Pure endoscopic approaches provide excellent access to the
ethmoid roof, cribriform plate, and most of the sphenoid sinus
60.
GRAFTS
• The specificdetails of graft selection have generated
considerable controversy.
• Potential grafts include
• Temporalis fascia,
• fascia lata,
• muscle plugs,
• pedicled middle turbinate flaps (mucosa alone or mucosa and
bone)
• autogenous fat
61.
• free cartilagegrafts (from the nasal septum or
the cartilaginous auricle)
• free bone grafts (from the nasal septum or
calvarium as well as other sites).
• Vascularised flaps(nasoseptal flaps and
turbinate flaps, lateral nasal wall flap that
involves the inferior turbinate and nasal floor
mucosa
62.
• Grafts areused for the following
functions:
(1) to fill a space through mass effect
(2) to re-create a watertight layer
(3) to act as a rigid buttress
(4) to stabilise a wound edge
63.
• The selectionof grafting material largely depends on the
availability of the material and the experience and
preference of the surgeon.
• Interest in the use of xenogeneic collagen dural
substitutes for example, Durepair Dural Regeneration
Matrix, DuraGen Dermal Graft Matrix , and Dura-Guard
Dural Repair Patch -for closure of skull base defects has
increased, due to advances in the endoscopic
management of complex skull base pathology, which
results in relatively large skull base defects.
• The collagen implant provides a scaffold for the native
fibroblasts to produce a collagen layer that blends and
eventually replaces the implant.
64.
• Ideally, graftsof fascia (or similar materials) should be
placed on the intracranial side of the defect with use
of an underlay technique.
• Mucosal grafts should never be placed intracranially,
and care should be taken to ensure the correct
placement, which avoids inadvertent intracranial
placement.
• Ambient ICP serves to hold the graft in position.
• Larger defects may require a layered reconstruction
including solid support such as cartilage or bone grafts
placed in the epidural space
• After the grafts are placed, a surgical sealant (such as
fibrin glue) may be used to help hold them in place.
65.
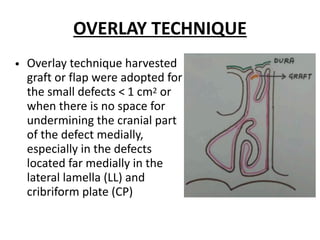
OVERLAY TECHNIQUE
• Overlaytechnique harvested
graft or flap were adopted for
the small defects < 1 cm2 or
when there is no space for
undermining the cranial part
of the defect medially,
especially in the defects
located far medially in the
lateral lamella (LL) and
cribriform plate (CP)
67.
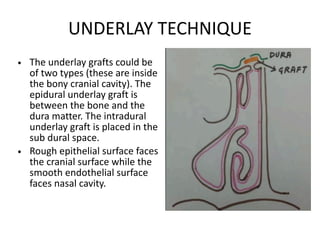
UNDERLAY TECHNIQUE
• Theunderlay grafts could be
of two types (these are inside
the bony cranial cavity). The
epidural underlay graft is
between the bone and the
dura matter. The intradural
underlay graft is placed in the
sub dural space.
• Rough epithelial surface faces
the cranial surface while the
smooth endothelial surface
faces nasal cavity.
68.
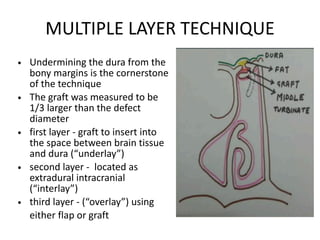
MULTIPLE LAYER TECHNIQUE
•Undermining the dura from the
bony margins is the cornerstone
of the technique
• The graft was measured to be
1/3 larger than the defect
diameter
• first layer - graft to insert into
the space between brain tissue
and dura (“underlay”)
• second layer - located as
extradural intracranial
(“interlay”)
• third layer - (“overlay”) using
either flap or graft
70.
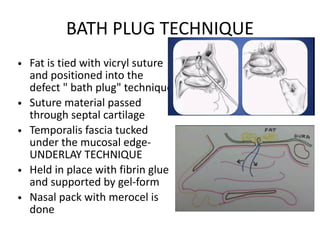
BATH PLUG TECHNIQUE
•Fat is tied with vicryl suture
and positioned into the
defect " bath plug" technique
• Suture material passed
through septal cartilage
• Temporalis fascia tucked
under the mucosal edge-
UNDERLAY TECHNIQUE
• Held in place with fibrin glue
and supported by gel-form
• Nasal pack with merocel is
done
71.
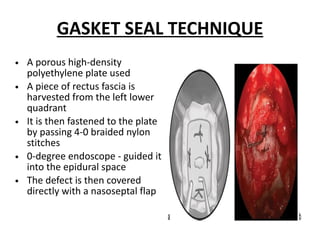
GASKET SEAL TECHNIQUE
•A porous high-density
polyethylene plate used
• A piece of rectus fascia is
harvested from the left lower
quadrant
• It is then fastened to the plate
by passing 4-0 braided nylon
stitches
• 0-degree endoscope - guided it
into the epidural space
• The defect is then covered
directly with a nasoseptal flap
72.
POST OPERATIVE CARE:
• Strict bed rest with the head of the bed elevated
• Soft diet and antitussives
• Broad-spectrum intravenous antibiotics
• Acetazolamide (ACTZ) for 4 weeks
• Sprays twice daily for 6 to 8 weeks.
• Minimizing their daily activity like weight lifting,
upstairs, sex, avoid constipation by eating rich fiber
diet, and avoid blowing their nose.
• Debridement of the skull base reconstruction
commences 4 weeks after surgery
• Monthly visits till 6 months
73.
COMPLICATIONS OF UNTREATEDCSF
RHINORRHEA
• Meningitis - 3-11 % risk within first three weeks after
trauma, overall risk 25%, with 10 % mortality, more
with delayed CSF fistula, MC organism isolated is
Pneumococcus
• Pneumocephalus - 20-30 %, including life-threatening
tension pneumocephalus- indicates open
communication with significant risk of meningitis and
encephalitis
• Cerebral Abscess
• Encephalitis
• Headache
74.
COMPLICATIONS OF CSFLEAK REPAIR
• Meningitis
• Pneumocephalus
• Brain abscess
• Epidural abscess
• Subdural abscess
• Intra cranial bleeding
• Postop Infection
• Formation of scar tissue in sinuses - c/o Nasal
obstruction
























![CSF rhinorrhea in Craniofacial Trauma[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/csfrhinorrheaautosaved-260206163910-49592e6e-thumbnail.jpg?width=640&height=640&fit=bounds)






























